Birth Control is Bad News for Thyroid and Liver

A lot of things baffle me about the medical industry’s approach to birth control, but the one thing I’ve struggled with the most has to do with the thyroid. For the life of me, I couldn’t understand how any doctor could prescribe The Pill to a patient and not be concerned about the affect it was having on the young woman’s thyroid.
The most frequent side effects experienced by women on birth control precisely mirror the symptoms of hypothyroidism: weight gain, water retention, constipation, irregular spotting, decreased libido, high cholesterol…
I believed one would have to be willfully blind not to see the connection. Then, I learned about another type of blindness in Daniel Kahneman’s book, Thinking, Fast and Slow.
Blind to Hypothyroidism
Kahneman won a Nobel Prize for his seminal work in behavioral economics. In the book, he describes numerous ways our minds process information and the, sometimes illogical, ways we respond to particular situations. A couple of the cognitive processes he details could help explain why doctors tend to overlook birth control’s affect on the thyroid.
First, what the author calls “a general ‘law of least effort’ [that] applies to cognitive as well as physical exertion.’ He says we have a laziness built into our nature, and once we learn a skill, we utilize fewer regions of the brain and consume less energy when we perform the task. Consequently, we are less engaged (Page 35).
The second factor has to do with attention. Kahneman explains, “When waiting for a relative at a busy train station, for example, you can set yourself at will to look for a white-haired woman or a bearded man, and thereby increase the likelihood of detecting your relative from a distance.” However, by focusing your attention on spotting this relative, you will miss other details – and not just the mundane.
To demonstrate just how focused we can become on a task, he cites the Invisible Gorilla study, which achieved notoriety beyond the realms of behavioral science because it seems so impossibly absurd:
“[The researchers] constructed a short film of two teams passing basketballs, one team wearing white shirts, the other wearing black. The viewers of the film were instructed to count the number of passes made by the white team, ignoring the black players. This task is difficult and completely absorbing. Halfway through the video, a woman wearing a gorilla suit appears, crosses the court, thumps her chest, and moves on. The gorilla is in view for 9 seconds. Many thousands of people have seen the video, and about half of them do not notice anything unusual. It is the counting task – and especially the instruction to ignore one of the teams – that causes the blindness. No one who watches the video without the task would miss the gorilla.” (Pages 23-24)
Likewise, if a new patient, who hadn’t recently started on The Pill, presented the same symptoms, no doctor would miss the warning signs of a hypoactive thyroid.
Focus on You
Doctors, through their training and experience, are intimately familiar with the side effects of hormonal birth control. So when a patient develops common complications soon after starting The Pill, skilled doctors believe it to be normal. They may suggest the symptoms will go away with time or may choose to prescribe a different formulation. Since they already know the source of the symptoms, the solution seems reasonable. It would be unnatural for them to consider the onset of an iatrogenic illness. After all, who keeps looking for the TV remote once they’ve found it?
This compartmentalization bias is precisely why a woman should trust her body more than the doctor when it comes to birth control. It’s not a coincidence that many women’s side effects resemble hypothyroidism (such as Hashimoto’s Tyroiditis), nor is it a coincidence that so many women develop a hyperactive thyroid (such as Grave’s Disease) soon after they stop The Pill.
Thyroid Under Attack
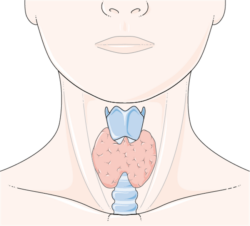
A normally functioning thyroid’s primary role is to produce two hormones known as T3 and T4. Produced in much smaller quantities, T3 is the active hormone, which regulates our energy, metabolism, and internal ‘thermostat.’ T4 could be thought of as T3 in waiting. It is produced in larger quantities so that can be delivered throughout the body, where it will be converted to T3.
Each cell in the body contains receptors for the thyroid hormones. These receptors remove a single iodine molecule from the T4, transforming the T4 into active T3. Thanks to this little miracle of chemistry repeating itself in every system of our body, the thyroid affects nearly every bodily function. Consequently, so does anything that disturbs that delicate balance.
Hormonal birth control creates myriad problems for the thyroid, beginning with the depletion of vital nutrients such as magnesium, selenium, zinc, and essential B Vitamins, like folate. The thyroid needs these important nutrients, especially zinc and selenium, to convert T4 to T3. Unfortunately, no amount of supplements will help your body overcome this obstacle.
While depleting nutrients, birth control also elevates production of Thyroid Binding Globulin (TBG). This protein binds with thyroid hormones to carry them through the blood stream, but renders them unable to attach to cell receptors. Consequently, the body may try to compensate by overproducing T3 and T4, without actually increasing hormone activity. This could explain why some women develop Grave’s Disease after stopping The Pill. Their TBG levels return to normal, but their body continues overproducing T3 and T4.
The Path to Long-term Fatigue
Women taking hormonal contraceptives have also been shown to have a three-fold increase in C-Reactive Protein (CRP), a widely recognized inflammation marker. The liver kicks into overdrive producing CRP in response to the inflammation associated with the birth control. This inflammation serves as a double-whammy to the already struggling tandem of the thyroid and liver.
First, the inflammation makes your cell walls less responsive to all hormones. Second, it disturbs the process of deiodination, leading to the overproduction of another inactive hormone known as Reverse T3 (RT3). As the name suggests, RT3 is the mirror image of T3, meaning the iodine molecule has been removed from the opposite side of the hormone.
RT3 competes with T3 for the same receptors. Since it is inactive, too much RT3 will leave you feeling lethargic. Your body responds by producing more cortisol in an attempt to boost your energy. If this continues for too long, it could lead to adrenal suppression, and long-term fatigue.
Weighing on the Liver
So, what causes this inflammation in the first place? As the central organ in the metabolic process, the liver produces proteins, breaking down fat and hormones to generate energy. When we overload the body with an unnatural flood of factory-produced, artificial hormones, the liver becomes sluggish and inefficient. This sets off a toxic cascade of side effects that leads to inflammation, and could ultimately contribute to chronic illnesses such as heart disease, cancer, and autoimmune disease.
The National Institutes of Health were concerned about hormonal birth control’s affect of the endocrine system from the very early days. When Dr. Philip Corfman, the Director of the Center for Population Research, testified at the Nelson Pill Hearings in 1970 on behalf of the NIH, he warned that The Pill decreased the liver’s ability to change and dispose of certain chemicals, even decreasing its ability to excrete bile.
Their studies from the 1960’s showed that up to 40% of women on oral contraceptives experienced some changes in thyroid function. They made the connection that this had also contributed to changes in adrenal gland function, citing increased cortisol levels. Reading from the NIH report he helped author, Dr. Corfman said:
“Although it is not yet possible to draw definite conclusions about their effect on the health of women and infants, the use of these agents warrants close observation and surveillance. Effects of special concern include alterations in carbohydrate metabolism, the character and distribution of lipids, liver function, protein metabolism, and the development of hypertension as well as alterations of endocrine function.”
Congress followed up on the hearings with a special report issued in 1978. Beyond concerns addressed in the original hearings, the new Congressional Report discussed more hepatic complications associated with The Pill, including the ‘greatly increased risk’ of developing an otherwise rare form of benign liver tumor known as hepatocellular adenoma (HCA). (Page 36) Studies at that time showed that women who had taken The Pill for eight years or more suffered a 500-fold increased risk of developing HCA, with 4% of those becoming malignant.
Good News First
The good news is that many of the side effects of hormonal birth control are reversible, if you stop taking them soon enough. Not every person who experiences symptoms of a hypoactive thyroid will develop Hashimoto’s Thyroiditis. While environmental factors are pivotal in triggering the development of this chronic disease, you must also be genetically predisposed in order to be susceptible to Hashimoto’s or any other autoimmune disease.
The bad news is that a LOT of people are genetically predisposed to Hashimoto’s Thyroiditis. In fact, it is considered the most common autoimmune disease, at 46 cases per 1,000. An estimated 20 million Americans have some sort of thyroid disease, and Hashimoto’s Thyroiditis makes up about 90% of those with hypoactive thyroids.
Don’t ignore the 800-pound gorilla in the room. Please think twice about the potential complications before starting any form of hormonal contraceptive, especially if Hashimoto’s Thyroiditis, Grave’s Disease, or any other autoimmune disease have made their way into your family’s history.
The FDA approved The Pill despite it not being proven safe. Today, it has been linked to everything from blood clots and cancer to lupus and Crohn’s disease — and still has not been proven safe.
This book explores the medical and historical disconnects that brought us to this point.
Last updated on October 21, 2023 at 9:38 pm – Image source: Amazon Affiliate Program. All statements without guarantee.
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, like it, please help support it. Contribute now.
Yes, I would like to support Hormones Matter.
Image credit: UCI UC Irvine/Flickr.
This article was published originally on




You might be interested in