
One Fateful Day – And a Journey into the Enigmatic World of Thyroid Related Problems Begins
I remember the day of March 19, 2010 very well. That was the last day I ever went jogging. That was the last day I could have hopped on my bike and ridden 50 miles if I wanted to. That was the last day I ate my favorite breakfast of a 3-egg omelet topped with cheese and veggies, with 3 pieces of whole wheat toast slathered in butter and jam, 3 pancakes on the side, and at least a quart of milk. That was the last day I worked in my profession, brought home a paycheck, and was self sufficient financially. It was the day before I started taking Ciprofloxacin, a fluoroquinolone (FQ) antibiotic, for a simple UTI. And it was the last day I was a normal person with a normal life.
By March 25, 2010 – six days later — I was completely bedridden with severe pain in what felt like every tendon in my body, along with peripheral and central neurological symptoms and other symptoms from the side effects of that drug. These adverse effects are collectively called “Fluoroquinolone Toxicity Syndrome” (FQT), or “floxed” for short. And although I didn’t realize it then, my physical, professional, financial, and personal life as I knew it was over. Within a few days and a few pills, I joined the ranks of the chronically disabled, those with “chronic invisible illnesses”, and “Romney’s 47%”. It’s five long years later, and I still struggle with the aftermath of taking those few pills. I regret every single day since then that I ever even considered a fluoroquinolone antibiotic for a simple UTI.
So what does all this have to do with the thyroid gland? Well, like most victims of this toxicity, all my extensive traditional medical testing during the acute phase of the reaction, as well as for the first year and a half after, gave normal or negative results. Astoundingly enough, despite being severely disabled and feeling essentially non-functional, according to the medical profession, I was the picture of health on paper. Until I finally decided to do more than a TSH test to check my thyroid status. That’s when I discovered I had all the anti-thyroid antibodies. And that’s really when my journey into the enigmatic world of “thyroid problems” began in earnest.
Having the antibodies for both Hashimoto’s Thyroid Disease and Grave’s Thyroid Disease makes for an astounding array of symptoms. Many of them appeared to mimic or overlap my symptoms of Fluoroquinolone Toxicity. Naturally, as a result of these observations, and my experiences with these conditions, I started questioning as to how much fluoroquinolone antibiotics caused severe endocrine disruptions, in particular of the thyroid axis.
The Thyroid Fluoroquinolone Epidemic: Where Is the Research?
There is a lot of published research available showing how damaging the FQ’s are too many different body systems and cellular processes, but almost none of it includes the thyroid system or the endocrine system in general. I suspect that someday, studies will be published showing the association between fluoroquinolones and thyroid abnormalities. Until then, it will be up to patients themselves to try and figure out if this association exists for themselves. In my case, my suspicions were further strengthened when I found that thyroid hormone medications, both T4 and T3, dramatically and profoundly affected all my floxing symptoms. Even more interesting to me, iodine alone did the same. I also found it interesting that a significant number of flox victims reported hormonal disruptions of all types post flox, such as with sex hormones, adrenal hormones, thyroid hormones, dysglycemias presumably in association with insulin hormone, and Vitamin D, which is also considered a hormone. This was also true of me after I was floxed. Eventually, I created a website* summarizing my observations, experiences, interpretations, and hypotheses on these possible correlations.
I had several intentions in creating the website, and one of them is to start the conversation about this potential link between fluoroquinolones and thyroid related problems, hopefully leading to unbiased studies and research in this area. I believe it is sorely needed. According to the U.S. Preventive Services Task Force Clinical Guidelines:
“The annual number of dispensed prescriptions of levothyroxine sodium in the United States increased by 42% over a 5-year period, from 50 million in 2006 to 71 million in 2010. In 2013, there were more than 23 million new prescriptions and refills for a single name brand of thyroid hormone in the United States, making it the most commonly prescribed drug in the country.”
This implies there are a lot of “thyroid problems” out there. According to several news investigations airing across the country, the FQ antibiotics are one of the top five drugs prescribed in the US each year. In our current day and age, we are bombarded by many substances which are known or suspected endocrine disrupters, including affecting the thyroid system. Could the epidemic of FQ usage be contributing to the epidemic of thyroid-related problems resulting in patients receiving thyroid medication for life? It would not surprise me if this were the case. I hope association studies, along with causation studies, will be done someday. Until then, those of us with thyroid disorders are on our own in looking at FQ antibiotic usage history and questioning this association for ourselves.
In my case, it was pretty clear cut that the acute symptoms I experienced right after starting the antibiotic were actually caused, or at a minimum, triggered by the antibiotic. My flox symptoms were pretty classic for these reactions all around, and there is plenty of research, as well as anecdotal stories, to substantiate this. But were my symptoms also “thyroid related”? In other words, did the antibiotic affect my thyroid system, either primarily and directly, or secondarily through a “cascade effect”, and at least some of these floxing symptoms I experienced were actually “thyrotoxic” symptoms as well? I think the answer is yes. These are the issues that I explore in my website, and I will briefly present here.
Tendon Pain and Ruptures: A Link between FQ Antibiotics and Endocrine Disorders?
One of the most well known adverse effects of FQ antibiotics are tendon problems. Most flox victims will experience some level of tendon pain at some point in time during their flox reaction. Regardless of what other symptoms occur with FQT, the severe tendon pain that can occur, sometimes with resultant ruptures, is distinctive, idiosyncratic, and unique to FQ antibiotic use alone. It is a hallmark of FQT. So much so, that an FDA “Black Box Warning” about it exists for all fluoroquinolone antibiotics.
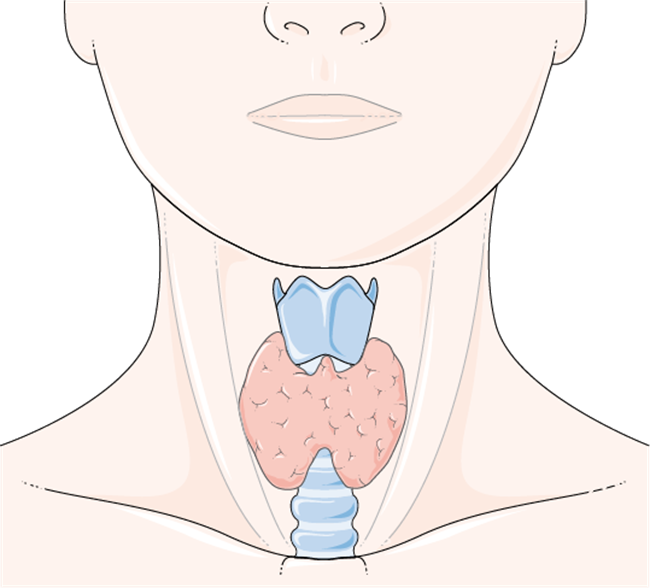
It turns out there just aren’t a whole lot of things in life, either natural or synthetic, that can cause sudden spontaneous tendon ruptures or severe tendon pain and tendinopathies –but all of the endocrine disorders can. This includes: hyperadrenocorticism (cortisol), diabetes (insulin), parathyroid disorders (calcium/PTH/Vitamin D), hyper and hypothyroidism (tyrosine/iodine/thyroid hormone), hyper/hypo sex hormones (estrogens/testosterone), and probably other steroid and sex hormones and their metabolites as well (see references). A specific genetic metabolism disorder of tyrosine, which is a major component of thyroid hormones, can also cause spontaneous tendon rupture later in life as a first manifestation of this disorder. Many rheumatic diseases also often have an associated, if not underlying, endocrine component (especially thyroid related). Additionally, conditions that at first glance appear to be unrelated, such as chronic renal failure, often have a high association with endocrinopathies, in particular, parathyroid hormone abnormalities. The parathyroid glands are intimately associated with the thyroid gland via proximity alone; if thyroid gland architecture is destroyed, presumably these glands could be affected too.
I took a fluoroquinolone antibiotic and developed severe, systemic tendon pain, Type 2 Diabetes, and two Autoimmune Thyroid Disorders. A legitimate question could be: Are fluoroquinolone antibiotics severe endocrine disrupters, which, among other symptoms, can result in tendon pain, tendinopathies, and tendon rupture?
I then found that the thyroid hormone medications T4 and T3, as well as iodine alone, profoundly affected my tendon pain and other symptoms, capable of making these symptoms dramatically better — or much worse. This, too, seemed to support the argument that the fluoroquinolones had somehow damaged my thyroid system, as supplying exogenous hormone in the form of medication now could make such dramatic differences in my symptoms.
One of my hypotheses is that people with healthy and normally functioning thyroid glands or other endocrine systems can probably withstand these dramatic changes in the hormonal axes that may be occurring while on the FQ – at least, up to a point. For people who don’t react at all to these drugs, they probably never even feel the fluctuations, as their hormonal axes can automatically adjust rapidly. But I would suspect that anyone with any underlying genetic predisposition, or possibly harboring a subclinical, latent, or silent endocrinopathy might be “pushed over the edge” into full blown clinical pathology. This is actually what I think may have happened with me, even though I had no overt indications of any kind of thyroid or endocrine disorder prior to taking the Cipro.
Additional Links To Consider Relating Fluoroquinolones to Thyroid System Damage
I don’t profess to even begin to know the millions of ways fluoroquinolones could possibly exert their damaging effects on the thyroid or endocrine system in general. However, that didn’t stop me from thinking about this problem. As I said, I hope research studies will be initiated in this area sooner than later. In the meantime, I came up with several mechanisms of FQ-Induced Thyroid Pathology to consider as possibilities, to narrow down the search. Additional unintentional targets of fluoroquinolones that I considered could have thyroid-related repercussions included targets such as mitochondria, acetylcholine, steroid receptors and hormone response elements and their common pathways, selenium dependent enzymes and proteins, halogenated peroxidase enzymes, iodine receptors located on most or all cells as well as on the thyroid gland, and more. I think one of the more interesting observations is the fact that new fluoroquinolone derivatives are now being considered for use as “tyrosine kinase inhibitors” (TKI’s). TKI’s are relatively recent chemotherapy drugs developed to fight cancer – and one of their adverse effects appears to affect the thyroid system with some rather alarmingly high statistics. From my perspective, there appeared to be striking similarities between thyroid abnormalities occurring with TKI’s and the thyroid abnormalities I suspect may occur with the FQ’s.
Fluoroquinolone Antibiotics: Consider the Risks
Thyroid disorders, especially autoimmune based ones, are no joke. Autoimmune Thyroid Disorders are not simply disorders of the thyroid gland; in my opinion, they are systemic disorders, affecting many or all of the cells and tissues in the body, which is why there can be such widespread and potentially devastating symptoms. There are numerous environmental stressors that contribute to thyroid disease and endocrine disease, and the fluoroquinolone antibiotics may be one of them. Fluoroquinolones exert many damaging effects, and if they are damaging the thyroid axis directly or indirectly via a cascade effect, actually causing anti-thyroid antibody production, or even if they are triggering or unmasking a subclinical or silent condition in susceptible patients to an active pathological condition, this is of serious concern – or it should be. A “silent” condition means just that – you don’t know you have that predisposition. I can say from my own experience that taking a fluoroquinolone antibiotic is a hell of a way to find out. It is Pharma’s responsibility to provide adequate warnings and risks of this possibility, and the medical profession’s responsibility to make sure adequate testing rules out these antibodies along with other potential risk factors, before prescribing a fluoroquinolone antibiotic. Sadly, neither of these things is happening right now. Until it does, I think anyone considering taking a fluoroquinolone antibiotic for a simple infection, such as uncomplicated UTI or sinusitis, should be aware of the risk factors and possible alternatives.
Based on what I’ve learned in the past several years, I believe anyone with pre-existing endocrinopathies of any type (whether they’re known or not), to be at increased risk for these adverse reactions. I also believe that anyone who has experienced any kind of flox reaction has now gotten a warning sign, and is at increased risk of developing an overt or clinical endocrinopathy as a result of being floxed at any time after. One of the few supportive pieces of evidence for this hypothesis is buried in Table 3, Page 136 of a Mayo clinic paper here. Note the at risk population includes people with autoimmune or endocrine disorders (diabetes, thyroid, parathyroid) and steroid usage (ie, Prednisone, inhalers, anabolic steroids, etc.).
The best approach, of course, is to stay away from these drugs altogether if at all possible. In my opinion based on my own experience, developing a lifelong severe thyroid disorder – or any other disorder — to solve a short term problem such as an uncomplicated infection with a fluoroquinolone antibiotic, isn’t worth the risk.
References and Resources
- Musculoskeletal Complications of Fluoroquinolones: Guidelines and Precautions for Usage in the Athletic Population
- The Risk of Fluoroquinolone-Induced Tendinopathy and Tendon Rupture: What Does The Clinician Need to Know?
- Spontaneous rupture of Achilles tendon: missed presentation of Cushing’s syndrome.
- Spontaneous rupture of Achilles tendon and Cushing’s disease. Case report.
- Incidence and predictors of hospitalization for tendon rupture in type 2 diabetes: the Fremantle diabetes study.
- Musculoskeletal Complications of Diabetes
- Biomechanical Properties of Achilles Tendon in Diabetic vs. Non-diabetic Patients.
- Spontaneous and serial rupture of both Achilles tendons associated with secondary hyperparathyroidism in a patient receiving long-term hemodialysis.
- Simultaneous chronic rupture of quadriceps tendon and contra-lateral patellar tendon in a patient affected by tertiary hyperparatiroidism.
- The level of vitamin D in the serum correlates with fatty degeneration of the muscles of the rotator cuff.
- Parathyroid disease.
- Primary hyperparathyroidism due to atypical parathyroid adenoma presenting with peroneus brevis tendon rupture.
- Thyroid hormones and tendon: current views and future perspectives. Concise review.
- Thyroid hormones increase collagen I and cartilage oligomeric matrix protein (COMP) expression in vitro human tenocytes.
- Suspected role of ofloxacin in a case of arthalgia, myalgia, and multiple tendinopathy. (Inhaled steroids and moderate hypothyroidism precipitating factors).
- Could Low Total and Free Testosterone Levels be risk factor for Achilles Tendon Ruptures in Males.
- Pathological rupture of the distal biceps tendon after long-term androgen substitution.
- Effect of estrogen on tendon collagen synthesis, tendon structural characteristics, and biomechanical properties in postmenopausal women.
- Female Athletes with Higher Estrogen Levels May Have Higher Injury Risk.
- Effect of administration of oral contraceptives in vivo on collagen synthesis in tendon and muscle connective tissue in young women.
- Successive ruptures of patellar and Achilles tendons. Anabolic steroids in competitive sports.
- Spontaneous rupture of the anterior cruciate ligament after anabolic steroids.
- Spontaneous rupture of the extensor pollicis longus tendon after anabolic steroids.
- Spontaneous tendon ruptures in alkaptonuria.
- Rheumatic manifestations of endocrine disease.
- The endocrine system and connective tissue disorders.
- Same Disease, Different Symptoms: It’s all in the Mitochondria.
- Your Mighty Mitochondria.
- Department of Health and Human Services Public Health Service Food and Drug Administration Center for Drug Evaluation and Research Office of Surveillance and Epidemiology Pharmacovigilance Review. (References provided for mitochondrial toxicity within the document).
Share Your Story
If you have been injured by a fluoroquinolone antibiotic, please share your story. Send us a note here, for more information.
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, like it, please help support it. Contribute now.
Yes, I would like to support Hormones Matter.
Laboratoires Servier, CC BY-SA 3.0, via Wikimedia Commons
*The website is no longer available.
This post was published originally on Hormones Matter on May 7, 2015; links have been updated where appropriate.













{kind=link}
Morning sunshine was very healing to me. It’s been over 10 years since Ive been floxed and I’ve seen so much healing. General vitamins (without additives) are healing as well, B vitamins, D, K, E…
Flouride bromides displace iodine. Dr Brownstein and Dr Dean Wilson and others discuss how iodine gets displaced and how iodine can displace the toxic halogen. T3 therapy in addition or instead of T4, iand / or iodine and selenium and l-tyrosine may help. The drs part of the iodine project. Iodine have positive effects on many glandular tissues according to info I read or heard.
I think this article is interesting. These antibiotics are horrible. The correlation between their use and increase in thyroid issues makes sense.
We really need to be cautious about what we take into our bodies. There are many dangerous medications but I believe these are among the worst. Some believing the mitochondrial DNA is getting messed up from the antibiotics breaking the DNA.
Very happy to see this web site. Thank you for that.
I’m the Doctor which has worked on this topic since years
Prof. Francesco Oliva (MD; PhD)
Professore Associato in Ortopedia e Traumatologia
Department of Musculoskeletal Disorders, School of Medicine and Surgery, University of Salerno, Salerno, Italy.
Dottore (PhD) in Ricerca delle Malattie dell’Apparato Locomotore presso Università degli Studi di Roma
“Tor Vergata”
Vice-Presidente I.S.Mu.L.T.
Associate Editor of MLTJ
olivafrancesco@hotmail.com
http://ismult.com
http://mltj.online
Combined ascorbic acid and T3 produce better healing compared to bone marrow mesenchymal stem cells in an Achilles tendon injury rat model: a proof of concept study
Francesco Oliva, Nicola Maffulli, Clarissa Gissi, Francesca Veronesi, Lucia Calciano, Milena Fini, Silvia Brogini, Marialucia Gallorini, Cristina Antonetti Lamorgese Passeri, Roberta Bernardini, Rosella Cicconi, Maurizio Mattei, Anna Concetta Berardi
J Orthop Surg Res. 2019; 14: 54. Published online 2019 Feb 18. doi: 10.1186/s13018-019-1098-9
Combined supplementation of ascorbic acid and thyroid hormone T3 affects tenocyte proliferation. The effect of ascorbic acid in the production of nitric oxide
Viviana di Giacomo, Martina Berardocco, Marialucia Gallorini, Francesco Oliva, Alessia Colosimo, Amelia Cataldi, Nicola Maffulli, Anna C. Berardi
Muscles Ligaments Tendons J. 2017 Jan-Mar; 7(1): 11–18.
Epidemiology of the rotator cuff tears: a new incidence related to thyroid disease
Francesco Oliva, Leonardo Osti, Johnny Padulo, Nicola Maffulli
Muscles Ligaments Tendons J. 2014 Jul-Sep; 4(3): 309–314.
Thyroid hormones and tendon: current views and future perspectives. Concise review
Francesco Oliva, Anna C. Berardi, Silvia Misiti, Nicola Maffulli
Muscles Ligaments Tendons J. 2013 Jul-Sep; 3(3): 201–203. Published online 2013 Aug 11.
Thyroid hormones increase collagen I and cartilage oligomeric matrix protein (COMP) expression in vitro human tenocytes
Anna C. Berardi, Francesco Oliva, Martina Berardocco, Marina la Rovere, Patrizia Accorsi, Nicola Maffulli
Muscles Ligaments Tendons J. 2014 Jul-Sep; 4(3): 285–291
Thyroid hormones enhance growth and counteract apoptosis in human tenocytes isolated from rotator cuff tendons
F Oliva, A C Berardi, S Misiti, C Verga Falzacappa, A Iacone, N Maffulli
Cell Death Dis. 2014 Jul; 5(7): e1329. Published online 2014 Jul 17. doi: 10.1038/cddis.2014.319
Metabolic diseases and tendinopathies: the missing link
Francesco Oliva, Silvia Misiti, Nicola Maffulli
Muscles Ligaments Tendons J. 2014 Jul-Sep; 4(3): 273–274. Published online 2014 Nov 17.
Dr. Oliva, would you like to write for us, translate some of the journal articles for the lay audience. I am certain that you would reach a broad audience that is hungry for this type of information.
I am 3 years post flox from Cipro and am still con erned about my thyroid and adtenal glands. What are the best tests for thyroid function? I want to be sure I am getting the most accurate picture of my body’s functioning, and to be honest, most doctors don’t get it! Thank you!
Hi Lisa,
See links below. These are the tests I list on my website. TSH, fT4, and fT3 are the standard. However, I do recommend testing for thyroid antibodies as a priority if you haven’t already done so, as they can affect these three values, in particular TSH as I mention in “TSH and T4: Useful or Useless?” Ruling out an autoimmune component can be very helpful in deciding what actions, if any, you want or need to take regarding thyroid issues.
As you can see, I list additional tests as well for people who want a more comprehensive look and can afford the testing. It is difficult to get physicians to order these tests, in part because they’d have to justify the cost to insurance companies. So if you’re interested in the more extensive testing, you’ll most likely be “Testing On Your Own — When the Docs Refuse”
Thyroid and Parathyroid Related Testing http://fluoroquinolonethyroid.com/book_page/endocrine-tests-for-flox-victims/thyroid-and-parathyroid-related-testing/
Cortisol Related Testing http://fluoroquinolonethyroid.com/book_page/endocrine-tests-for-flox-victims/cortisol-related-testing/
TSH and T4: Useful or Useless? http://fluoroquinolonethyroid.com/book_page/t3t4-basics-some-key-points-2/tsh-and-t4-useful-or-useless/
Testing On Your Own — When the Docs Refuse http://fluoroquinolonethyroid.com/book_page/what-to-do/testing-on-your-own-when-the-docs-refuse/
I hope this is helpful!
Best,
JMR
Are there any resources for success in reversing the damage of fq & thyroid disorders? Any help would be so greatly appreciated! I took a mere five days of this poison, and being already hypothyroid at the same time, and on a thyroid hormone replacement that was not working at the time…I’m a mess and need solutions, this is going on two years for me, and getting worse.
Hi Krysti,
I’m very sorry you are going through this. Unfortunately, I don’t have any concrete and proven solutions to either thyroid or FQ related problems that will work for everyone. It’s been seven years since I was floxed, and there still are no good research studies done on the effects of FQs on any part of the endocrine system either. So those of us with problematic thyroid issues, or flox issues, or both, are still on our own in trying to find things that will help us. However, as you’re probably aware, there are multiple websites and forums dedicated to thyroid issues, and flox issues, where patients discuss numerous approaches to try and what has or has not helped them. I provided links to some of those sites on my website (sidebar). I was aware when I wrote up my website that I couldn’t provide proven solutions, and so I always direct people to those other websites in the hopes they will find something there that works for them. Until or unless the scientific research and medical communities get on board and figure out some definitive answers, these patient-driven resources are the best we have available to us. I would encourage you to keep looking, and keep trying, and I really wish you the best.
My heart was beating rapidly within 3 days of taking cipro. I lost 10 pounds in 12 days. I had no heart palpitations prior to taking the antibiotic. 2 months later I’ve been diagnosed with advanced Graves’ disease (an autoimmune disorder) and it’s recommended that I have my thyroid taken out. I think it is linked to the cipro,
Hi Dianne,
I’m very sorry this has happened to you. Your post makes it sound like your case of hyperthyroidism is very recent, and that you took Cipro about 2 months ago. If this is the case, there is a chance that your symptoms of hyperthyroidism might be transient in nature, and that you may be able to manage your symptoms and quiet down the thyroid gland without surgery. I discuss why this is in several places on my website, but I know my website is long and may be hard for you to understand if you are new to thyroid disease.
If your symptoms are tolerable right now, I would recommend taking some time to research the internet about Graves disease and hyperthyroidism using a more natural approach. I did a Google search on “Graves Disease Natural Treatments” and numerous sites came up. People have successfully managed their Grave’s Disease without surgery, so I think these are options that should also be looked into before making any decisions. I provide a few of the links below that might be a little easier to understand.
Once your thyroid gland is removed, there is no going back. If your symptoms are tolerable, or you can learn to manage them, it can buy you time to at least look at all the options available for treatment and give your thyroid gland a chance to recover from the Cipro insult. However, Grave’s disease can be quite serious, with the threat of “thyroid storm” and eye problems. I am not saying you will experience this, but it’s important to realize this is a possibility and this is why you need to start learning as much as you can about Grave’s and the variety of approaches used to help with it. It’s also for this reason that I would very much recommend searching out a functional or holistic doctor that is aware of all the natural as well as conventional options for treating Graves to help you. Maybe you’ll eventually need your thyroid gland removed. But if there’s any chance you can save your thyroid gland, it will be worth it.
https://drruscio.com/natural-management-graves-disease/ Natural Management of Grave’s Disease.
http://www.elaine-moore.com/Articles/Graves%E2%80%99DiseaseArticles/WhatstheRushinTreatingGravesDisease/tabid/169/Default.aspx What’s the Rush in Treating Graves’ Disease?
http://gravesdiseasecure.com/ Graves’ Disease Natural Treatment
http://fluoroquinolonethyroid.com/wp-content/uploads/2014/11/FQ-Story-quotes-7-thyroid.pdf Scroll down to “Darby’s Story” to see how “Darby” appears to have successfully used bugleweed for diagnosed Grave’s after taking Cipro. (Please note that I cannot recommend the caffeine, although obviously it either helped or at least didn’t hurt Darby’s recovery. However, FQs are also known to damage caffeine metabolism, and I know that many people, including me, can no longer tolerate any caffeine as a result).
For the more science oriented who might be reading this, search PubMed for “hyperthyroid bugleweed”, “hyperthyroid L-carnitine” and “hyperthyroid selenium” to learn how these natural substances can help tame an overactive thyroid gland as effectively as some of the conventional medical treatments.
Hi,
I had a Hysterectomy with A LOT of complications in November 2015. After I was released a week later I came down with a fever. I was admitted to the hospital with an infection on the inside of where my surgery took place. After a CT scan, I was told that they would need to put me on several HIGH doses of antibiotics to kill the infection or have to go through my back to remove the infection. After 48 hours of iv antibiotics (it’s all I could smell and taste, it was horrible) my infection was gone. Almost 2 years later, I found a Holistic doctor that treats you off of your blood test results, not your symptoms. My test results showed that my white blood cells are elevated, high TSH, low FT4, low Ferritin, extremely low B12, low FT3, extremely low Vit D, DHEA Sulfate is high, Serotonin is extremely low and my Pregnenolone is low. I’ve gained 30 pounds (and can not get rid of it) and I have a laundry list of other issues. Before I had surgery I worked out and had plenty of energy and never weight problems. My question is could all the antibiotics they had me on caused this???
It’s likely a combination of the two factors. Hysterectomy alters hormones significantly, while the antibiotics induce and/or exacerbate nutrient deficiencies. Both affect thyroid function directly and indirectly.
Hi Crystal,
I’m very sorry to hear of your health troubles. I agree with Chandler, that it could be a combination of the two factors, and possibly additional factors we’re not aware of that may have developed in the years since the hysterectomy. I hope your holistic practitioner attempts to address your current symptoms, using your blood work as a supportive guide, and that you’re able to get some healing help with these issues!
JMR, I’ve been reading through your site and writings. First of all, thank you for your generosity in sharing your experiences and all the information you’ve acquired along the way. I am so sorry for the ordeal you’ve endured and am inspired by your fortitude. I fear my 14 year old daughter is experiencing similar symptoms. I know her serum iodine levels were extremely low 2 months after she began experiencing FQ reaction. She was a competitive swimmer and exposed to lots of fluoride and chlorine and maybe bromine throughout the years. She is currently functionally disabled, not even going to school regularly. I’m having trouble finding a professional to look at the big picture and help put her on the path to healing. Do you have recommendations for the sort of doctor/specialist/expertise we should try to find? Need someone who understands the thyroid, FQ damage, and delicate balance of biochemicals at play. I’d like to share your findings with someone who understands the science behind all this — but what sort of professional would that be? Endocrinologist believes FQ toxicity is unlikely.
Hi Laura,
I’m so, so, so sorry to hear of your daughter’s health issues! I hope that she is able to find help and healing! Here is a doctor referral list that has doctors that are recommended by other people who have been adversely affected by fluoroquinolones – http://floxiehope.com/2013/12/11/doctor-referral-list/. Progressive Medical Center in Atlanta, Georgia has also helped many people, and comes highly recommended. If none of the doctors on the list, or Progressive, work out for you, functional medicine doctors seem to approach things in a way that is healing – https://www.functionalmedicine.org/practitioner_search.aspx?id=117. Also, this page from JMR’s site should be helpful http://fluoroquinolonethyroid.com/book_page/what-to-do/why-test-and-dear-doctor-letters/. Also from JMR on http://fluoroquinolonethyroid.com/book_page/get-to-the-point/ –
” I believe that once a person has been floxed, they may always be at greater risk for thyroid problems. As such, I do recommend a thorough thyroid panel, in particular the autoimmune component, be tested for in the acute phase and monitored for several years post flox. This is true for people already on thyroid hormone medication as well (continual monitoring of the autoimmune antibodies despite being on thyroid hormone medication). Current clinically available anti-thyroid antibody testing includes: TPO, TgAb, TSI, TrAb, and TBII. The TSI, TrAb, and TBII are every bit as important as the TPO and TgAb, and possibly more so during the acute phase. It is not enough to only test TSH, T4, or maybe TPO. I also recommend a traditional spot urine iodine test during the acute phase of FQT, as well as continual monitoring. I highly suspect that people with low iodine status are susceptible to FQ reactions. For those so inclined, testing for minerals during the acute phase would be a good idea; I would include Selenium, Zinc, and Copper in this testing.”
I hope those things help!
Regards,
Lisa Bloomquist
Hi Laura,
My apologies for responding so late; I did not see your post. I am so incredibly sorry to hear of what your young daughter is going through. I sincerely hope she has improved since your post.
I am glad that Lisa responded to your post when she did and I think she provided you with some good information, at least, as far as anyone knows so far when it comes to FQT/FQAD. Unfortunately, as you are aware, it is extremely difficult to find medical or research professionals to look at the big picture. It’s beyond frustrating to me that this is the case. I wish I had more definitive action to recommend for victims, but until more research is done, we’re all in the same boat, on our own, trying different things to see what helps and what doesn’t.
That is interesting that your daughter’s serum iodine levels were extremely low after she began experiencing an FQ reaction. I hope more people continue to test for iodine levels, either serum or urine, so we can start getting a more objective idea of how often this is occurring with FQT/FQAD. The urine iodine spot test is a simple test that can be ordered without a physician and done at home, so I recommend it.
If you haven’t checked for this in your daughter, I also would like to reiterate testing for calcium/PTH for possible parathyroid adenomas. As you may have seen, there is currently a discussion on Lisa’s Floxie Hope site by a woman who appears to have recovered from all her FQT/FQAD symptoms by having the surgery for this. Most importantly to note is that, as is too often the case, none of her doctors thought her calcium levels, which were normal but fluctuating in the higher ranges, were a problem. She took matters into her own hands, referred herself to the physician surgeons who are experts in this particular condition, and woke up after a 20 minute surgery with most, if not all, of her symptoms gone. There are not many chronic conditions with widespread symptoms full of suffering that can be cured with a quick surgery, but this is one of them that has that potential. Your daughter is young, and will most likely have naturally higher levels of calcium, and I’m guessing physicians therefore won’t look any further into this possibility. As to how likely it is that a 14 year old girl might have a parathyroid adenoma, I don’t know (and admittedly, mainstream medicine would say ‘very unlikely’). But the fact is, you won’t know until you check, it’s a simple blood draw and a relatively inexpensive test to run, and therefore pretty easy to rule in or out. So I would encourage you to do this in the interest of “leaving no stone unturned” in your quest to help your daughter.
You are probably aware of these pages since you’ve read the site, but I’ll post the links again for others who might be reading as well:
http://fluoroquinolonethyroid.com/book_page/endocrine-tests-for-flox-victims/thyroid-and-parathyroid-related-testing/ Lists the specific thyroid and parathyroid tests
http://fluoroquinolonethyroid.com/book_page/what-to-do/testing-on-your-own-when-the-docs-refuse/ Discusses how most people in the US can bypass needing a physician and order these tests on their own if they want.
Again, my apologies for not seeing your post sooner, I hope you will read this. I also hope that “Kathy”, the other poster diagnosed with a parathyroid disorder, will also see this. I don’t know what type of abnormal parathyroid function tests Kathy had, but if it was high calcium and PTH, then I hope she will realize she has options which could be helpful to her situation.
My heart breaks to hear of what your daughter and you are going through. I sincerely wish I could have found real answers to these problems, and could help you both more. People do recover, and your daughter has youth and a motivated parent on her side. Best of luck to both of you.
If you have brain fog and memory problems. Read about chemo-brain – this is exacly what happened to me after cipro – CHEMO _ BRAIN FOG. This often happen after anticancer medication!! Cipro is neurotoxic like anticancer drugs. Read about chemo-brain and you will find this happen to you unfortunatelly 🙁 Only meds that can help : psichostimulant drugs like modafinil, methylfenidate and maybe donepezil.
Selegiline can help too , improve cognition – yes this antiparkinsoniana drug. IN higher dosage it is antidepresant – iMAO B and A.
I took cipro for 2 weeks. Stright after treatment ends I got very strong brain fog and memory loss. I feel like my brain stop thinking I got anxiety, cant drink coffe now I get high blood pressure etc, I is 1 month after being floxed. Why they still prescribing these poison to people. Please report any adverse reaction to proper institutions.
I’m new to this. I has received fluoroquinolone antibiotics several times without known difficulties. Both levofloxacin and ciprofloxacin. Problems began after I received IV levofloxacin in the hospital for pneumonia. The pneumonia cleared up but I was left feeling exhausted and sleeping around the clock most days. My nurse practitioner did a series of lab tests and my TSH (thyroid stimulating hormone) and parathyroid hormone function tests came back abnormal. I was prescribed levothyroxine but was reluctant to start taking another medication. I looked online and that was the first time that I suspected that I had been “floxed”. I’m less clear on what the parathyroid abnormality symptoms will be, as well as what other endocrine effects will be. I can tell you that as a RN I am very frightened about the potential negative effects will be on my life. I never received any warnings other than to take it easy so as not to cause tendon rupture. I don’t think the doctors had any intent other than to cure my pneumonia, and previous treatment for UTIs. Now what to do? I’m waiting to talk to my NP to advise her of this info so that she and my physician can advise me.
Hi Kathy,
I am so sorry you are going through this. I know it is a frightening experience.
Kathy, that is very interesting that you had PTH tested and it came back abnormal. I wish every person during the acute phase of being floxed, or when tendon issues occur, would run the parathyroid tests, even if total calcium is normal. We might find out if there is an association between PTH abnormalities and flox symptoms. So I think it’s great that your NP included it in her testing.
I don’t know if you’ve visited my website or not, but I discuss the thyroid and parathyroid testing here. If TSH is all you’ve had done so far for thyroid, I would recommend doing the more extensive testing:
http://fluoroquinolonethyroid.com/book_page/endocrine-tests-for-flox-victims/thyroid-and-parathyroid-related-testing/
Having said that, I wish there was more I could offer you in terms of what to do next. Everybody’s case is so different, and many different approaches exist, as I’m sure you’re already finding out from reading the internet. There are many very informative websites, forums, and support groups for thyroid, parathyroid, and floxing. I would recommend learning all you can from them, as well as talking with your NP and physician. Take it a step at a time, try not to get too overwhelmed, and speak with people you trust before making any big decisions.
Also it is very frightening to find out you may have been “floxed”, but please realize that people do get through this and recover. I was particularly hard hit, but your case may be very different from mine. There’s no reason right now not to think you’ll recover. Hang in there and best of luck.
Fluor supress thyroid funcion. Ciprofloxacin and thyroid function:
A growing number of studies have revealed that neurocognitive impairment, induced by adult-onset hypothyroidism, may not be fully restored by traditional hormone substitution therapies, including thyroxine (T4):
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4262484/
Ciprofloxacin interacts with thyroid replacement therapy:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC557149/
Evaluation of the effects of ciprofloxcin or gatifloxacin on neurotransmitters levels in rat cortex and hippocampus::
http://www.academicjournals.org/app/webroot/article/article1380811746_Rawi%20et%20al.pdf
Exploration of the Neurotoxicity of Ciprofloxcin or Gatifloxacin Single Dose in Rat Cortex and Hippocampus:
http://www.researchgate.net/profile/Nadia_Arafa/publication/272265313_Exploration_of_the_Neurotoxicity_of_Ciprofloxcin_or_Gatifloxacin_Single_Dose_in_Rat_Cortex_and_Hippocampus/links/54e0709f0cf2953c22b4aa4a.pdf
All this happened to me.I was doing all right until I was prescribed cipro.
The fluoroquinolones should be taken off the market and publicly incinerated.
These drugs wrecked my life.
Lucy