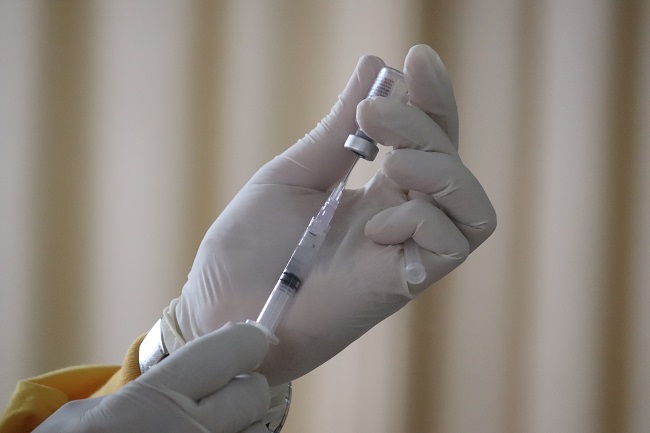

Leuprolide, more commonly known as Lupron, is the GnRH agonist prescribed for endometriosis, uterine fibroids, cysts, undiagnosed pelvic pain, precocious puberty, during infertility treatments, to treat some cancers, and a host of other off-label uses. It induces a chemical castration in both women and men. In women, Lupron stops menstruation and ovulation and crashes endogenous estradiol synthesis rapidly and completely, inducing menopause and menopause-associated symptoms like hot flashes, sweats and osteoporosis, to name but a few. In men, where it is used as a treatment for prostate cancer, it prevents the synthesis of testosterone, pharmacologically castrating its users and evoking a similar constellation of symptoms.
Lupron for Endometriosis: Questionable Research
Lupron’s widespread use for pain-related, female reproductive disorders, such as endometriosis or fibroids is not well supported, with little research indicating its efficacy in reducing pain and no research delineating its effects on disease progression. Conversely, evidence of safety issues have long been recognized, especially within the patient communities where reports of chronic and life-altering side effects are common. We have many case reports on our site alone. Although, class-action and marketing lawsuits have arisen, Lupron continues to be mis-prescribed regularly to diagnose or treat pelvic pain disorders like endometriosis, generating over $700 million in revenue in 2010 and 2011 for the manufacturers and an array of serious and chronic health issue for its recipients.
The reported side effects of Lupron are staggering both in the breadth of physiological systems affected and the depth of symptom severity experienced (a partial list). Indeed, everything from the brain and nervous system to the musculature, skeletal, gastrointestinal and cardiac systems are affected by Lupron, sometimes irreversibly. This is in addition to thyroid, gallbladder and pancreatic side effects. How can one drug evoke so many seemingly disparate side effects? Is it possible that the magic of chemical castration is not as safe as we were led to believe; and that hormones regulate a myriad of functions beyond reproduction? It is.
Beyond Reproduction and Reproductive Disease
A major fallacy in medical science, and indeed medical research, is the total compartmentalization of physiological systems and by association an insoluble marriage of hormones to their respective reproductive organs, functions, and gender. Lupron, and drugs like it, were developed based upon this fallacy; that somehow suppressing estradiol and the other endogenous estrogens would affect solely the reproductive system. If only human physiology were that simple.
Hormones, even those inappropriately designated sex hormones, like estradiol and testosterone, regulate all manner of physiological adaptations in every tissue and organ in the body and they do so in conjunction with other hormones and by decidedly non-linear trajectories. That is, the dose-response functions are curvilinear where both too little and too much of a particular hormone can evoke serious negative consequences in body systems totally unrelated to reproduction. Chemical and surgical castration would fall into the ‘too little’ category.
Hormone Receptors are Ubiquitous
Hormones mediate these reactions via hormone receptors. Estrogen and androgen receptors are located throughout the brain and the nervous system, on the heart, in GI system, in fat cells, in immune cells, in muscle, the pancreas, the gallbladder, the liver, everywhere. When hormones bind to these receptors, whether they are membrane bound, nuclear, or other types, the hormone-receptor complex activates or deactivates what are called signal transduction pathways, essentially message lines. Those messaging lines tell the cell to do something. Too much or too little of any one type of hormone sends mixed messages, skewing cell behavior just slightly at first and when there are only small changes in hormone concentration, but with more chronic or more severe hormone changes, the signals become increasingly more deranged and the compensatory reactions, meant only for short term, become more exaggerated and self-perpetuating. This is where problems emerge. Even if estradiol or more appropriately, estrogens (there are many estrogens) feed endometriosis, tanking estradiol concentrations is dangerous and sets into motion complex reactions that we are only now beginning to understand.
Hormones Influence Everything
Since the hormones and receptors are broadly located throughout the body, it doesn’t take a genius to figure out that if we kill off one or more hormones completely, as Lupron does with estradiol, there are going to be negative effects globally, and they are likely to be pretty serious. So, even a surface level evaluation of the safety of drug like Lupron, would suggest a strong possibility of negative outcomes in regions of the body not associated with reproductive function. And with just a little bit of endocrinology under one’s belt, it should be clear that negative outcomes would compound over time, as additional reactions meant to compensate for short term changes in hormone concentrations, become increasingly entrenched and self-perpetuating, and in many cases, increasingly damaging to the health of the cells – but it isn’t. Despite the range of serious side effects, Lupron is a commonly and cavalierly prescribed drug and newer versions of Lupron like drugs are expected to take the market by storm.
Estradiol Is Critical to Human Health
While the pharmacological mechanism of action for Lupron and drugs like it is clear, they override pituitary control of the tropic hormones that signal the ovaries or testes to synthesize new hormones, how these drugs induce the array of side effects, many of them long term and even permanent, has not been explored as seriously as it should be. Certainly, one can hypothesize the effects of estradiol elimination on different systems based upon receptor distribution within each tissue and the signaling pathways therewith, but the effects are diverse and sometimes contradictory or highly tissue specific. One has to wonder if there might be a final common pathway by which the elimination of estradiol could disrupt multiple physiological systems in a predictably discriminate manner. Indeed, there might be.
Estradiol Regulates Mitochondrial Function: Mitochondria Regulate Everything Else
If you’ve read any of our articles over the last year, you’re aware that we have become increasingly interested in mitochondria, particularly how drugs and nutrients or nutrient deficiencies, impact mitochondrial functioning. Mitochondria take nutrients from food we eat and convert them to the biochemical energy required to power cellular life – ATP. Without appropriate cellular energy all sorts of things go wrong. Energy is fundamental to life and so functioning ATP pathways are critical for cellular and organismal health (and so is proper nutrition!). A number of disease states emerge when the mitochondria are damaged or inefficient at producing ATP, from chronic fatigue, muscle wasting and autonomic system dysregulation to name but a few. Estradiol, and likely other hormones, (most of the research focuses on estradiol), influences mitochondrial functioning and the production of ATP via a number of mechanisms.
Estradiol Is Needed for the Production of ATP
Though not a component of what is called the citric acid or TCA cycle or the electron transport chain (also called the mitochondrial respiratory chain), estradiol appears to be intimately involved in up – and down-regulating the enzymes and other proteins within those energy production cycles. Estradiol directly and indirectly modifies the types fuel used to produce ATP (glucose, fatty acids or proteins) and impacts the efficiency and flexibility with which ATP is produced. Essentially, estradiol impacts the substrate inputs and keeps the cogs in electron transport chain cycles moving. When estradiol is eliminated, fuel sources shift (by tissue) and those cogs, called complexes, begin to slow, become less efficient and send off more damage signals (reactive oxygen species – ROS) than can be effectively cleaned up. Since functioning mitochondria and sufficient ATP are required for cellular health in all cells, where energy demands are greatest, symptoms emerge: the brain and nervous system, the heart, the GI system, muscles, and bone formation/turnover.
In the brain, we see serious cognitive deficits and derangement of mood and perception with damaged mitochondria relative to estradiol elimination. We also see autonomic instability that impacts mood (flipping between depression and anxiety) but also heart rhythm and balance.
In the heart, the estradiol directly impacts mitochondrial fuel preferences and availability by regulating cardiac glucose and fatty acid metabolism. Without estradiol, the machinery within the mitochondria are not as flexible in their ability to switch between glucose, fat or proteins for precursor fuels to make ATP. The lack of flexibility, particularly during other physiological stressors, leads to impaired cardiac functioning and increased inflammation in affected tissues.
Bone formation is particularly hard hit as estradiol is required bone growth, maturation and turnover. Estradiol deficiency leads to increased osteoclast formation and enhanced bone resorption – destruction of bone or osteoporosis. Proper bone formation is also highly dependent upon vitamin D concentrations. Vitamin D deficiency leads to bone loss. Vitamin D activates estradiol synthesis, while estradiol activates vitamin D receptors. Lupron tanks estradiol and by association vitamin D, a double hit to bone health. At the level of the mitochondria, the third hit, reduced ATP, further damages bone health.
Estradiol is an Antioxidant
Antioxidants scavenge ROS. Antioxidants are needed to keep ROS concentrations at bay as too much ROS, though a natural byproduct of ATP production, will damage the mitochondria and initiate a damaging, self-perpetuating cycle. The body has a number of anti-oxidants to temper ROS. Many nutrients are included in this category: Vitamins C and E, CoEnzyme Q10 and glutathione are among the most well known. It turns out that estradiol and progesterone are potent anti-oxidants as well. So chemically or surgically eliminating estradiol reduces the body’s ability to detoxify and eliminate damaging ROS, evoking further mitochondrial damage.
Estradiol Modulates Mitochondrial Hormone Synthesis
That’s right, the mitochondrial estrogen receptors impact what is called steroidogenesis – steroid hormone synthesis – for multiple hormones, not just those pesky ‘female’ hormones. Like a thermostat that turns on or off when the temperature changes, mitochondrial estrogen (and other hormone) receptors sense hormone changes and up or downregulate the synthesis of pregnenolone (and the use of cholesterol to make pregnenolone). Pregnenolone is the precursor for all steroid hormones. So when Lupron or ovariectomy tank estradiol, not only is the synthesis of estrogens affected, but so too is the synthesis of other steroid hormones.
Estradiol Tempers Mitochondrial Ca2+ Homeostasis
Ca2+ balance is a complicated topic, a bit beyond the scope of this paper but is an important function modified by mitochondrial estrogen receptors. Ca2+ influx into cells is excitatory and turns on the cellular machinery. As one might expect, too much or too little Ca2+ activity could be damaging. Too much Ca2+ is cytotoxic or neurotoxic (if in the brain), killing the cells. The mitochondria are largely responsible for controlling the influx of Ca2+, sequestering Ca2+ when there is too much in order to save the cells. So when mitochondria become damaged or inefficient by any mechanism, Ca2+ homeostasis becomes an issue and cell death, tissue and organ damage become very real outcomes. Estradiol influences the mitochondria’s ability to sequester and temper Ca2+, so that the cells don’t become too turned on or over-active and die. (This is an interesting mechanism because estradiol itself is an excitatory hormone, increasing the activity of the cell when bound to the cell membrane or nuclear receptors but when bound to receptors on the mitochondria, estradiol tempers that excitation.)
Estradiol Regulates Immune Function
Estradiol bound to the estrogen receptors on immune and other cells activate and deactivate a number of signal transduction pathways that turn on/off inflammation and other immune responses. The mitochondria also regulate immune function via ROS signalling. Depletion of estradiol, particularly at the mitochondrial level, guarantees disrupted immune function and hyper inflammation by way of mitochondrial structural damage, derangement in function, and the loss of estradiol mediated anti-oxidant abilities. So by multiple mechanisms Lupron, drugs like it, and ovariectomy, damage mitochondria and initiate cascades of ill health.
Lupron, Maybe Not Such a Good Idea
Estradiol bound to mitochondrial receptors, controls a whole host of functions in the mitochondria, which then control cellular health throughout the brain and body. Without estradiol, the mitochondria become misshapen and dysfunctional and eventually die a messy death (necrosis), but not before inducing mutations in next generation mitochondria (mitochondrial life cycles include the regular birth of new mitochondria and the necessary death of old and damaged mitochondria). As the damage and mutations build and the ratio of healthy to damaged mitochondria shifts, cell death, tissue/organ damage and disease develop. Lupron, other drugs that tank estradiol, and ovariectomy, initiate mitochondrial damage. The mitochondrial damage represents a possible final common pathway by which Lupron induces the myriad of side-effects and adverse reactions associated with this drug.
A question that remains, is whether this damage can be offset by supporting mitochondrial machinery by other mechanisms. This is particularly important since millions of women have been exposed to Lupron and/or have had their ovaries removed. Other hormones and a myriad of nutrient factors are necessary for the enzymes within the mitochondrial machinery to work properly. Could we offset the damage evoked by too little (or too much) hormone by maximizing the efficiency of the other reactions. I think it is possible, at least theoretically and at least partially. That will be addressed in a subsequent post. For now, however, I think we ought to reconsider the use Lupron, other GnRH agonists, antagonists and the surgical removal of women’s ovaries. The damage evoked by eliminating estradiol is likely far greater than any potential benefit in an ill-understood disease process like endometriosis.
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, like it, please help support it. Contribute now.
Yes, I would like to support Hormones Matter.
Photo by Mufid Majnun on Unsplash.
This article was first published on January 16, 2015.












My life was forever altered by just one injection of this horrific poison. I remember being 24 years old, sitting in my OBGYN’s office and her telling me (after she had performed abdominal surgery to look around and confirm I had endometriosis, but did nothing else) that it was one of only two ways I could treat. The other being birth control pills. Oh if only I had the information I do now back then. One shot of this stuff and I had the most severe anxiety, panic and depression I’ve ever felt in my life. Thank goodness I decided on only one shot, but then did take oral Danazole (sp?) for about a month after, which essentially does the same thing as Lupron. I gave that up too and eventually decided to go on birth control. If I could go back to that scared girl in her 20s I would tell her to try some progesterone cream once the estradiol level started to build back up. All of my symptoms were from the abrupt stoppage of estrogen. I experienced this again last summer during peri/menopause brought on by trauma. I was 46 and my lab work showed menopause. I started on topical estrogen and progesterone and wow, what a difference. I will never be without bio identical hormones as long as I live.
My advice to young women who are getting diagnosed with endometriosis is this… please don’t take these GnRH agonists, EVER. Find a naturopathic/functional med doctor who will help you with bio identical hormone replacement. I’ve lost so many years due to these meds and the subsequent choices I made in order to stay in survival mode (anti-depressants and benzos). If my story helps just one other woman, it has been worth it to share.
I was on it for two years. The first two months I had complete anterograde amnesia but was not taken off of it. I ended up with permanent dystonic tremors that are considered fast progressing and twisting my body sideways, major depressive disorder moderate recurrent episodes, my hair is falling out, and I’ve just been having health problem after health problem. I just lost my ability to do my passion (dancing and martial arts) due to a high risk of injury. My lungs are being compressed. Seriously if anyone wants to study my brain and body by all means…
I am Japanese and had Leuprorelin Acetate injection in this September and have already read this paper.
In this review, you wrote that “The mitochondrial damage represents a possible final common pathway by which Lupron induces the myriad of side-effects and adverse reactions associated with this drug.”
I would like to confirm.
Do you think that the Estradiol synthesis damage represents a possible common pathway by which Lupron induces the myriad of side-effects and adverse reactions associated with this drug?
Thank you for your reply Dr Marrs, I expected last year to receive an edited version of my posts for it to be shared more widely but I didn’t receive the edited version…
Chandler Marrs, PhD says:
March 26, 2018 at 1:36 am
I will send you an email in a few days with the post so that you can review before we publish
Per this last communication I don’t understand your last answer to my comment. You did not get my email or you do not have my email address? Where should I send it if this is the case? Where should we go from here?
Thank you for your ongoing studies and connection!
Wow. Something must have slipped through the cracks. I do not remember the correspondence. My apologies. Would you resend the story and I will edit and prepare immediately. Again, I am so sorry that I dropped the ball here.
Synarel is equally as dangerous. I was prescribed it for IVF and it gave me a functional neurology disease. Almost a month using this spray i developed head vibration, vertigo and severe depression. These symptoms have been constant for the past 8 months and have causef me to have mental breakdowns. I am 33 years old.
Yeah right this drug is poison.Iwish Ihad never taking it.
Thank you!!!! You have no idea how happy it makes me to see someone talking about the benefits of estradiol. I get so sick of everything being about estrogen dominance and how we all need to lower our estrogen. I feel much better on estrogen than progesterone but now I’m post-menopause and there goes estrogen and my energy. It was also the start of my dysautonomia – vertigo, tinnitus, orthostatic hypotension, weird cold sensitivity, peripheral neuropathy. Exogenous estriol and estradiol give me energy, improve my mood and make my body feel stronger. A doctor gave me progesterone and it reduced my estradiol below the measurable level and caused health issues I’m still recovering from 3 years later.
“A question that remains, is whether this damage can be offset by supporting mitochondrial machinery by other mechanisms. This is particularly important since millions of women have been exposed to Lupron and/or have had their ovaries removed. Other hormones and a myriad of nutrient factors are necessary for the enzymes within the mitochondrial machinery to work properly. Could we offset the damage evoked by too little (or too much) hormone by maximizing the efficiency of the other reactions. I think it is possible, at least theoretically and at least partially. That will be addressed in a subsequent post.”
Can you please point me to the post where this is addressed? Or offer any suggestions on hormones or nutrients that might help – especially for a post-menopausal woman? I’ve been told get your adrenals right and magic will happen. Not so much. There’s a missing link somewhere. Could it be thiamine or is it something else? I know post-menopause there are limited options but I’d love to find something that will help. Taking exogenous estrogen isn’t an option without progesterone when you have a uterus and progesterone does the opposite of estrogen. It makes me a very unhappy miserable person with pain and increased vertigo and dizziness. Not much fun!
I hope to see more on the role of estrogen, progesterone and thiamine in mitochondrial health. I find it fascinating.
I was diagnosed with prostate cancer about 9 months ago. Since then I have under gone 9 weeks of radiation therapy and 7 months of hormone therapy with 2 months left. I have had a 3 month Lupron shot followed by a 6 month shot. I also have acromegaly with an active tumor, diagnosed in 1987. About 6 weeks ago, I started having deep depression, anxiety, and constant obsessive thoughts. I didn’t know what caused this and thought I was going insane. Eventually, I decided it was the Lupron and have had blood work done. All my hormone levels that have been checked so far are way off. My urologist and endocrinologist are finally starting to take this seriously. Knowing what I now know, I realize I should never have been considered a candidate for Lupron therapy with an existing pit. tumor. I will die of prostate cancer before I will ever take another Lupron injection.
My post was removed, it was not a joke, it was serious.
Maam,
My daughter was born through the IVF process and i think my then feed me IVF drugs she took during the processes. Is this still an active blog? And is there anyway i can make contact with to asks questions.
The reason i think my ex did this is from my working with primary care doctors that are confused by my symptoms and i have received no help. When searching syptoms i keep getting women having a hard time getting back after IVF treatment and men who were chemically castrated. Lupron was on of the drugs my ex possessed along with many more.
Since my server sickness with my ex wife and days of it, i have never regained phyically or in vitality.
I just do not know how to approach this due to primary care docs summarily bursh anything i say off and i have not talked about this with my VA (veteran adminstration) doc and have no clue how to do so.
Any help?
Yes, it is still an active blog. I am not sure I understand your questions. Were you given Lupron?
I received Lupron inections in 2011. Shortly after, I developed a rapidly growing pituitary tumor that ruptured. My life is forever altered. I’m on multiple medications for hypopituitarism. Not to mention, the pituitary tumor also caused complete menopause at the age of 30. All thanks to lupron a medication that was supposed to help me.
Becky. Do you work for Abbot? I am pretty sure you do!!
We are not talking about one or three victims here. we are talking about thusands of women and men, so please be respecful with our pain and go to the Pro Lupron page to talk about your succesful experience with this poison drug
Dear all,
In Europe the patient information leaflets changed. It now includes thyroiditis as a common side effect for woman. I don’t know if that also happened in the USA but I guess a lot of women around the world now know where their Hashimoto’s disease or Graves’ disease comes from.
So on the inserts for Lupron, thyroid disease is recognized in Europe?
For decades foreign labels for Lupron have identified “thyroid enlargement” as an adverse event – i.e. , 1995 Australian label (“Lucrin”). And as early as 1986 the US product label for the initial formulation of Lupron (1 mg. subcutaneous daily injection) identified “thyroid enlargement” as an adverse event; and the US product label for the intramuscular injection of monthly Lupron Depot 3.75 mg likewise identified warnings for thyroid adverse events … until these thyroid adverse events were removed from the US product label in 2005. As of today, no thyroid adverse event warnings are identified in the US label.
It is worthwhile here to revisit the atrocities committed during the only Lupron lawsuit to get to trial (Karin Klein v. TAP/Abbott, 2011). Karin, at age 17, was prescribed Lupron in 2005 when Lupron’s label no longer contained the prior-listed warnings about adverse thyroid events. Karin developed, among others, serious thyroid problems. Belatedly learning of Lupron’s prior US label warnings of adverse thyroid effects in US, as well as the prior and current similar warnings in foreign labels, Karin sued for failure to warn. The judge refused to allow the jury to learn of Lupron’s pre-2005 US labels warning of adverse thyroid effects; the judge refused to allow the jury to learn of Lupron’s past and current foreign labels identifying adverse thyroid events; and the judge refused to allow the jury to learn of published medical literature identifying Lupron’s adverse thyroid effects. The judge would only allow the jury to learn of the 2005 US label. Moreover, Abbott’s mendacious defense expert committed outright perjury by claiming “it was absolutely biologically impossible for Lupron to affect the thyroid gland”, while a simple PubMed search shows this “expert statement” to be absolutely false (ie, see the first published report, in 2000, to “demonstrate the association of thyroid disorder with leuprolide [Lupron]” – http://www.ncbi.nlm.nih.gov/pubmed/11228054).
This court’s curious restriction of limiting disclosure to only the 2005 Lupron label (devoid of any adverse thyroid warning) created the illusion for the jury that there were NO thyroid adverse effects for Klein to have been warned about — and so by a legal sleight of hand, Klein’s claim of “failure to warn” was made to disappear, and the jury found for Abbott. An appeal – bewilderingly – resulted in the Circuit Court misstating facts and making false statements, denying Klein her right to a fair trial. And the US Supreme Court refused to hear the case. These circumstances resulted in a devastating miscarriage of justice – not just for Klein, but for all Lupron victims (and someone in the legal arena should be examining the events in this trial). Further details on this case, and links to court documents, can be found @ http://www.lupronvictimshub.com/lawsuits.html (@ bottom of page, left column).
Lynne, this is a fantastic bit of information and with just a little more, an intro and conclusion, would make a great blog post. Any chance I can convince you to make this into a blog?
You have easily convinced me – I’ll forward an elaboration to you next week. And I will also clarify a point not made entirely clear in my post above: in 2005 all thyroid adverse effect warnings were removed from the US Lupron Depot (monthly) product label, however the US product label for the daily 1 mg subcutaneous formulation of Lupron continues to identify adverse thyroid warnings.
Thank you Lynne.
Yes.
This is interesting! I took Lupron 18 years ago after having taken Syneral many years earlier. I got a hysterectomy in 2005 and since then new problems have appeared. I currently have a diag. of Fibromyalgia for lack of anything more accurate, since 1998. Within the last few years I get episodes of thyroiditis with thyroid function fluctuating and hormone, natural or synthetic does not help, in fact it makes it worse, so Hashimoto’s is “suspected”. Doctors rarely know what to do with me, so it is a waiting game, as it has always been. A different kind of suffering….I’ve been following the mitochondria theory re: Lupron toxicity.
Connie, Our stories are so similar that it is scary. I took 6 monthly injections of 3.75 mg. Lupron 1996. Had to go on disability with a diagnosis of fibromyalgia, as well. Had a total hysterectomy with oopherectomy in 2003. Had to have a partial thyroidectomy in 2015 for a growing thyroid nodule with atypical cells. I also agree with you, that the fibromyalgia diagnosis is no more than given our pain, insomnia, chronic fatigue, mental anguish a name. Let me know if you have all these other symptoms? I miss the former person I was prior to Lupron toxicity. Thank you.
With my deepest gratitude to Dr. Marrs for her generosity and good will in providing this one stop shop for all those who are frustrated trying to get help from their specialists post Lupron AND DRUGS LIKE IT. I wish I could have just printed out this mammoth article to take to my GP and army of expensive specialists, who denied my extensive list of debilitating symptoms even existed, let alone explain or treat them seven years ago. Having my symptoms diminished or altogether denied in some cases was just as distressing as the undisclosed side effects themselves.
Briefly, “and drugs like Lupron”, I presume refers to other GnRH-a’s, including: Nafarelin (Synarel), Buserelin (Cinnafact, Suprefact, Metrelef), Goserelin (Zoladex), Triptorelin (Trelstar, Decapeptyl, Gonapeptyl), and Histrelin (Vantas, Supprelin LA). As a Synarel survivor, who suffered from profound short-term memory loss, chronic fatigue and abdominal pain, insomnia and vertigo (naming only the most distressing side effects) after my first and only IVF attempt, I am grateful for any mention “other drugs” like Lupron get, seeing there is even less information available for them. Utilizing a GnRh-a as part of a fertility treatment is a contraction in terms and crime against humanity.
Jacqueline, thank you for the kind words. I do my best. There is still a lot to learn. Regarding my use of ‘other’ meds, yes, I was referring to GnRH agonists but also the new breed of antagonists. We cannot forget surgery too. The removal of the ovaries has the same effect, permanently.
Dr. Marrs, I must deeply thank you for your work on this matter. Thank you, Lynne, as well for sharing your experience and work. Here is my story and I blame it all on the abrupt lack of “female” hormones. I am a non practicing physician. Now 45 y.o. I was 24 in 1997 when I had an acute abdomen due to a chocolate cyst that gave me the diagnosis of endometriosis. After surgery I was given 6 months of Lupron receiving one injection a month. This set me right away into chemical menopause. The worse adverse effect I had to deal with after the hot flashes that reversed once I started taking OCP as a treatment, was the PERMANENT EFFECT ON MY MUSCLES. Before this surgery and treatment with Lupron, I was doing fencing and even competed. I had done sports all my life till that point in which I was never again able to practice any activity or sport without pain during and days after the activity. After years of trying, it came to the point I needed medication to ease the pain and stiffness and talked to my PCP about my undiagnosed obvious fibromyalgia. I had a couple IVF treatments down the road without success before starting pregabalin along with tramadol added years later due to insufficient pain control.
The second part of my daily challenges came after a diagnosis of breast cancer in 2011 before age 40, having to undergo for a second time an artificially imposed menopause, this time due to chemotherapy followed by complete hysterectomy (which means ovaries were removed as well to diminish the chance of hormonal influence in a receptor positive cancer). HOT FLASHES are still with me 6 years after, day and night, every 40 minutes more or less, even long after finishing therapy with Tamoxifen. MUSCLE PAIN AND WEAKNESS have become so much worse since then. I blame it again on the sudden loss of “sexual” hormones which affect all tissues as we now know. I should also mention cognitive changes and periods of depression.
I’m aware that some diagnostics urge the need to take medications regardless of their adverse effects but it is EXTREMELY IMPORTANT TO KNOW THESE as to make a truly informed decision when it comes to choosing therapies. It’s a hard call “quality vs quantity in life expectancy” but we should have the right of choosing.
It would be wonderful to know more about all that happens to our tissues (“cell lungs”=mitochondria) due to these abrupt changes in hormonal levels along with their necessary actions, and to have a better educated medical community that can better relate to patients without ignoring the unique role they play in the life of their patients and the consequences these drastic treatments bring upon their lives.
Please let me know If you have received this message and if there is any other information I can collaborate with.
Cecilia, can we copy/paste/edit and turn your comment into a post so that it is shareable and more women will see it?
Sure, Dr. Marrs (or moderator?), you can do so as far as the content is not changed significantly and my personal email is protected. I’m happily surprised and pleased to see my message was acknowledged and valued.
I hope the junk mail I’ve received today in my email mailbox was not due to posting my view in this webpage.
I’d like to add that per my experience, having gone through menopause twice, once with Lupron and next with chemotherapy and hysterectomy, I believe that, in my case, at least part of the symptoms experienced post Lupron may be due to the sudden withdrawal of normally released sexual hormones and due to a postmenopausal state rather than due to the drug itself. The expected therapeutic effect for the condition being treated by the prescribing physician becomes, per my understanding, the nightmare of symptoms experienced by the patient due to the lack of time given to the tissues to adapt to the hormonal changes that happen in a drastic manner instead of in a tapering slope. These symptoms, experienced as a “hormonal withdrawal” by our body may then be interpreted by patients as being the adverse effects of the drug. By this, I’m not saying that Lupron may not have significant adverse effects, I’m just pointing out that we may confuse adverse effects of the drug with the permanent changes caused to our body due to the sudden disruption on the affected hormonal levels, or that there may be an overlap between these two.
Along the years, I’ve been more and more aware of the progressing fatigue, weakness, muscle/ligaments aches, stiffness, difficulty in performing daily cognitive tasks and keeping interest in a social life. All is interconnected and is a two way road. Once I started having fibromyalgia symptoms and others, it was first difficult to acknowledge objectively that something was indeed happening to my body that I could not control with will and training, next, I had to accept those changes and learn to cope with them, next I had to explain/convince my doctors that I did have a new condition that limited my life and that needed adequate medication just to get out of bed and go through a day like a “normal” person, next came explaining family and friends what made my daily struggle different from theirs… when your muscles burn just from going up few steps, or holding your arm up to change a radio station or browse a few garments at a store, you start being aware that can not be normal. When you need to take a 4 hours nap after going few minutes on a treadmill and bike with minimal speed and resistance or after going through a 6-7 hours period low energy demanding activities in your day, you start wondering this can not be normal…
Hopefully more can be learnt and done about our starving mitochondria and quick aging bodies in their functionality after these interventions that are given to us in hopes to remedy precaucious menopause, endometriosis, tumors and cancers in women and men.
Thank you for your daily efforts in trying to achieve this for us!
I will send you an email in a few days with the post so that you can review before we publish.
Hello, Dr. Marrs, it’s been almost a year since I wrote after reading your article. I would like to contribute with further research for example if tissue samples or more info about my case can be of use.
Unfortunately, I did not get any further email regarding an edited version of what I had shared on this web page with the intention or hope for it to be shared with more people.
Looking forward to read from you and any further related studies being carried on. Regards, Cecilia.
Cecilia, yes we would be interested in sharing your case story. I don’t recall seeing an email from you.
I took one injection of Lupron last month and am due for a second one next week. I opted for it because I was diagnosed with breast cancer, triple positive. Since I’ll need chemo, I wanted to protect my ovaries with Lupron. And they want to continue the Lupron after chemo so I can be rendered menopausl allowing me to take an aromatase inhibitor which works better than tamoxifen. I understand the importance of estrogen but if it feeds my estrogen receptor positive cancer cells, is it worth it to take Lupron? Plus an aromatase inhibitor? More quality of life to allow some estrogen to circulate despite it possibly feeding cancer cells?
Because of decades of my own research into All-Things-Lupron, I’d like to take this opportunity to not only thank Dr. Marrs for her interest and work on this paper and in this matter, but I’d also like to provide Dr. Marrs and anyone with interest some disturbing information on Lupron’s mechanism(s) of action (which is detailed below). This analysis by Dr. Marrs adds considerable and keen insight into the ‘how and why’ so many Lupron victims have suffered so much, and in so many bodily systems – and Dr. Marrs should be commended on her efforts and her analysis.
But first I’d like to address the commenter Becky’s viewpoint (“stop criminalizing this drug!”) and her support of Lupron. This position is quite misguided, and – as bizarre as it sounds – Becky and her doctor *should* be turning to the internet for accurate information on Lupron (as evidenced by the very posting of Dr. Marrs’ paper). In the event Becky has been in that infamous ‘Lupron fog’ all these years – she should be informed that there exists in excess of tens of thousands of Lupron victims, and thousands have been clamoring for years for an investigation (see http://www.petition2congress.com/1902/investigation-lupron-side-effects-leuprolide-acetate/). A minimum of reading on Becky’s part of other dire assessments of Lupron’s dangers, written by renowned physicians, should provide further cause for concern (See Dr. Redwine and Dr. Gueriguian’s expert testimony on Lupron’s risks @ http://www.lupronvictimshub.com/lawsuits/RedwineExpertReport001.pdf and @ http://www.lupronvictimshub.com/lawsuits/GueriguianReport.doc). Why isn’t Becky aware of these known and serious Lupron risks?
It is, of course, a good thing whenever hemorrhaging is being controlled, and Becky claims “if it wasn’t for [Lupron she] would be dead now”. However, I’ve spoken with mothers (note the plural) who would shiver in horror were they to hear this comment, for these mothers firmly believe their daughters (young women in their 20’s) would be alive today if it weren’t for their daughters’ Lupron injection.
I receive contact from men, women, and children (either the parent or grandparent, or the now-adult child) who suffer from serious, disabling, and permanent physical and mental adverse effects on and after Lupron (see excerpts of emails @ http://wp.rxisk.org/lupron-a-nightmare-produced-in-abbvie/), and there needs to be an army of medicolegal advocates to assist these victims, but there is not.
The number of years Becky has been ‘on and off Lupron’ is troubling. Lupron for women can only be administered for one 6-month course, though another 6-month course may be prescribed if a bone scan is performed and ‘add-back therapy’ is co-administered – for an absolute limit of 12 months total Lupron in a LIFETIME. Has Becky had a bone scan? Was Becky advised of alternatives such as blood transfusion and hysterectomy? If hysterectomy was not an option because of a desire for children, Becky should note that an independent review of Lupron’s endometriosis raw clinical trial data revealed 62.5% of women FAILED TO RETURN to baseline ovarian function one year after end of study, which is evidence of “long-term damage to ovarian function”. The drug company, however, alleges in its Lupron product label (which is used to “inform” doctors) that this same clinical trial data instead showed Lupron’s effects were “fully reversible” after stopping Lupron. (See “Hidden Clinical Data about Lupron” @ http://impactethics.ca/2014/05/02/hidden-clinical-trial-data-about-lupron/#more-1297 , and see “Lupron and FRAUDULENT DATA” @ http://www.lupronvictimshub.com/lawsuits.html).
Any transparent, comprehensive look into Lupron’s data and effects, the devastation from Lupron’s iatrogenic injuries, along with the marginalization of Lupron victims, should make clear the folly of declaring “stop criminalizing this drug!” and instead should raise a call to “start prosecuting the criminals!”
I’d like to elaborate upon Dr. Marrs’ statement that the pharmacological mechanism of action for Lupron “is clear”. While there is indeed voluminous literature asserting such claims, replete with detailed descriptions of the hypothalamic-pituitary-gonadal axis – in fact, the entirety of Lupron/GnRHa’s mechanism(s) of action remains “unclear”, “not known”, “not fully elucidated” and “not fully understood”. It is pertinent to quote here the FDA reviewer’s report on Lupron’s pharmacological and toxicological data in rat studies, prior to Lupron’s initial FDA approval: rat “testes showed various degrees of testicular degeneration … [t]he severity of the lesions were greater 7 days after cessation of treatment indicating that the effects continued after drug withdrawal … There are other inconsistent effects of Leuprolide in the various toxicology studies but potentially the most serious effect of Leuprolide, in my view, is its effect on spinal column bone marrow. This increased fat deposition and subsequent hypocellularity was explained as a physiological response to the drug. … … Leuprolide administration produced [] a two-fold increase in pituitary adenomas in both male and females … The sponsor’s explanation is that Leuprolide acts as a constant stimulator of gonadotroph function resulting in hyperplasia and ultimately, production of tumors. However, in the method and dose employed, Leuprolide does not stimulate but actually inhibits pituitary gonadotropin synthesis and secretion. Nevertheless, the possibility exists that Leuprolide at the same time may be acting as a stimulator of other cell functions which could result in pituitary adenomas. There is no obvious reason to suggest that the same process could not occur in humans. … [end of report redacted]” (see http://www.lupronvictimshub.com/home/USAdraft.doc @ pages 8-9).
Just months after the Arpril 1985 initial FDA approval of Lupron for human use, it was reported in a study of rats that “the inhibitory actions of GnRH in uterus may not involve estradiol receptors … GnRH analogs were found to have post-transcriptional effects” (http://www.ncbi.nlm.nih.gov/pubmed/2417040 ). Years after Lupron was approved for the indications of palliative treatment of prostate cancer and endometriosis, it was acknowledged that “no thorough evaluation of the effect of these substances on the pituitary, the site of supposed action, has been reported” (http://www.ncbi.nlm.nih.gov/pubmed/1459255), and after more than a decade of treating “endocrine-dependent cancers [with GnRHa’s], their biological mechanism remained obscure” (noting that results in this cancer cell line study provided evidence that GnRHa stimulation of ERK activity may not be mediated by extracellular Ca2+) (http://www.ncbi.nlm.nih.gov/pubmed/10537288).
In 1990, it was noted that “a direct effect of potent GnRH-analog on the central nervous system resulting in neurological effects independent of the hypothalamic-pituitary-gonadal axis is possible”. (Citations for this and all following quotes will be provided below). In 1993 a lead gyn Lupron investigator reported “The cause of some adverse effects reported has no clear endocrine mechanism … The mechanism of joint pain remains unclear and warrants further investigation … Two of the most disturbing adverse effects experienced by women receiving Lupron were depression and short-term memory loss. Although the mechanism of these symptoms are unclear, GnRH-a treatment should be discontinued if depression or short-term memory loss develops.” (One GnRHa/IVF study found “72%” experienced difficulty with memory – a majority of subjects). In 1995 “it [was] increasingly apparent that [GnRHa’s] do not just affect the gonadal hormones, but are powerful modulators of autonomic neural function.”
Lupron’s manufacturer, Lupron brochures, and Lupron-prescribing gyn physicians describe Lupron’s effects as “menopausal”, however it needs to be acknowledged that the hormonal profile of a menopausal woman (increased FSH/LH, decreased estrogen – “hypergonadotropic hypogonadism”) DOES NOT MATCH the hormonal profile of a woman on Lupron (decreased FSH/LH, decreased {sometimes} estrogen – “hypogonadotropic hypogonadism”). Similarly, Lupron is described to consumers as a “hormone”, “chemotherapy”, or “hormonal chemotherapy” – yet the ‘deHaen Modified American Hospital Formulary Service Therapeutic Classification System’ classifies Lupron within the category of “10:00.12 – Antineoplastic/OTHER” (along with Interferon and Mitotane), and does not classify Lupron within the category “10:00.10 – Antineoplastic/HORMONE” (which contains Tamoxifen and Flutamide). What is this “OTHER”? (Interferon is regarded as a “Biological Response Modifier”, and it is noteworthy that Lupron’s initial 1985 FDA approval for palliative treatment of prostate cancer was not approved out of the FDA’s ‘Office of Drugs’, but rather Lupron was approved out of the FDA’s “Office of Biologics Research and Review”.)
During Lupron’s approval for pain management of endometriosis, the FDA Medical Officer noted “It is difficult to understand why symptoms seem to decrease within two – four weeks of starting [Lupron], prior to even well-established hypogonadism and amenorrhea.” And note the comment of an FDA Medical Officer in review of Lupron for endometriosis prior to approval, in which it is stated “The most common adverse event was hot flashes, the majority of which occurred within 3 months *after* stop of study”. Women are told Lupron-induced hot flashes are caused by hypoestrogenism (low estrogen), yet women who have ‘escaped’ Lupron (having above-menopausal estrogen levels), women who are on ‘add-back therapy’, and women who have stopped Lupron *continue* to experience hot flashes. One researcher concluded these hot flushes have nothing to do with estrogens but rather that “dysregulation of the GnRH releasing clock center in the nucleus arcuatus in the mediobasal hypothalamus is associated with altered central alpha-receptor activity which results in lowering of the set point of the central thermostat and the circulatory changes.”
Is the molecular weight of leuprolide (Lupron) “1209.42” as stated in published medical literature, or is the molecular weight of leuprolide (Lupron) “1269.47” as stated in published medical literature? Is Lupron “metabolized by enzymes in hypothalamus and anterior pituitary” with a “half-life of 3 hours” as stated in published medical literature, or is Lupron metabolized by being “destroyed within the GI track” with a half-life up to “4.25 hours” as stated in published medical literature, or does Lupron have a half-life of up to “6.8 hours” as stated in published medical literature?
(Citations for all quotes and information within the above 4 paragraphs are found in http://www.lupronvictimshub.com/docs&corr/LUPRNSUQok.doc @ #’s 3, 4, 9, 11, 15, 49, 69, 71, 72, 74, 77, 78, 79, 82, 92, 115, & 142. See also http://www.lupronvictimshub.com/USAdraft.doc @ Section “III. HAVE TAP, INVESTIGATORS, AND PHYSICIANS REPORTED ACCURATE AND FULL DATA REGARDING LUPRON?”. See also “NLVN Factsheet – Lupron: Mechanisms of Action and Probes” @ http://www.lupronvictimshub.com/NLVN.html ).
When “little [was] known about the effects of GnRH agonists on the hypothalamic-pituitary-adrenal axis”, 10 women on GnRHa’s were studied with the subsequent conclusion that the use of GnRHa’s “does not apparently alter the hypothalamic-pituitary-adrenal axis” (see http://www.ncbi.nlm.nih.gov/pubmed/8380603). Ten women are studied and a conclusion is allowed to be drawn – yet tens of thousands of Lupron victims’ complaints are deemed “anecdotal” and have been essentially dismissed by the majority of the medical community?!
Over the years I have seen articles about gonadotropin-induced LOSS of hormone receptors and also the increasing numbers of various tissues that contain GnRH receptors – and, admittedly, much of this subject is beyond my comprehension, but red flags do stand out. In short, ALL OF THE ABOVE begs so many questions and concerns, and I echo your precautionary advisement to “reconsider the use of Lupron, other GnRH agonists, antagonists and the surgical removal of women’s ovaries”, and have previously called for a ban of Lupron. And indeed, in 1989 an FDA Medical Officer involved with Lupron’s approval for endometriosis had her own cautionary advisement about Lupron: Dr. Ragavan advised using “even more caution in this [young female] population” than the “extreme caution” “always used” in rendering men hypogonadal (“reserved … for life threatening conditions in the male”), because these young women “must live with the consequences of treatment for a very long time.” (See http://www.lupronvictimshub.com/USAdraft.doc @ pages 11-12). (I can envision those aforementioned mothers [plural] interjecting here in unison: “… IF they live.”).
The interest, research and analysis undertaken by Dr. Marrs is sorely needed and greatly appreciated, and I hope the information provided above can be helpful in some way. I look forward to the future posting on this subject, and I sincerely wish that Dr. Marrs’ work and analyses will stimulate further medical, academic, scientific, and judicial interest.
Lynne Millican, RN, BSN, paralegal (disabled post-Lupron)
Founder, Lupron Victims Hub
http://www.LupronVictimsHub.com
Thank you Dr. Marrs, for offering a scientifically-sound view of some of the potentially dangerous systemic effects of GnRH antagonists.
I have personally spoken with several women who developed severe and PERMANENT, almost crippling side effects, immediately after beginning Lupron therapy.
This drug is NOT always prescribed for life-threatening diseases and every success story shouldn’t be used for blanket denialism of the horrors that drugs like Lupron can inflict in some cases.
stop criminalizing this drug! Just because you may have not felt this drug helped you doesn’t mean that it hasn’t helped others. Listen to your doctors they will suggest what works for you. Every medication has side effects if you read the side effects from tylenol or gravol you would never take it. I have been on and off Lupron for years and it is the only drug that has been effective in stopping my menstral hemraging I bled for 8 months straight with no relief from other drugs. Lupron was given to me by my doctor and stopped the bleeding and their for stopped the spread of the disease. If it wasn’t for this medication I would be dead now due to blood loss. It was not possible for my body to replenish the blood it was losing. I have been on Lupron for 5 years off and on and now I am on it again. Yes the hot flashes are a little uncomfortable but I would take them any day over the hemraging. So before you believe what is on the Internet talk to your doctor and know that this drug DOES help people, and that it is not always just about the bad stories you read.
Some drugs work for some people. But not others. I went through two years of hell from one injection of Lupron. My weight dropped to 83 pounds from a healthy 132. I stopped menstruating. To date I’m unable to shake the severe depression this drug caused. It’s been twenty two years and it’s unlikely I will ever recover fully. Glad it worked for you but don’t demonize those of us who suffered from the darker side of this drug. For us, it’s poison.