Every woman dealing with endometriosis has faced this question at some point in her journey. It may be a question she has asked herself, as she navigates treatment options, perhaps having tried many treatments that have not worked. Perhaps her doctor has stated it as the only possible next step. Or, friends and family members have suggested it, thinking that it is a cure for endometriosis. Sometimes, endometriosis patients feel pressured by those around them to consent to this surgery. And sometimes endometriosis patients are so desperate to find a solution to the never-ending pain that they just want “everything out” and to not have to deal with it anymore.
Does Hysterectomy Cure Endometriosis?
If you are considering a hysterectomy to manage endometriosis pain and symptoms, the first question that needs to be asked is how effective is a hysterectomy in curing endometriosis? There have been some studies published that address this question. The rate of symptom recurrence varies quite a bit depending on the study—from 19 to 62 percent, when at least some ovarian tissue was conserved. One major reason for persistent pain after hysterectomy for endometriosis is incomplete removal of endometriosis lesions at the time of hysterectomy, and thus, the reason for the variability between the studies likely reflects, at least in part, the differences in surgical skill at completely excising all endometriosis lesions.
What about Removing the Ovaries?
When both ovaries and both Fallopian tubes are also removed at the time of hysterectomy (bilateral salpingo-oophorectomy, or BSO), the risk of symptom recurrence is lower, but still present, at 8 to 10 percent. Again, complete removal of endometriosis lesions at the time of hysterectomy improves post-operative outcomes.
Many endometriosis patients who have had hysterectomies and bilateral oophorectomies for endometriosis are reluctant to take hormone replacement therapy (HRT) for fear of stimulating any endometriosis tissue that may have been left behind. This question has not been addressed comprehensively with published studies. The risks of HRT related endometriosis growth depend somewhat on whether any endometriosis tissue was left behind at the time of hysterectomy. The risks of HRT in general, however, cannot be dismissed. Studies have shown a higher incidence of certain cancers, gallbladder disease and cardiovascular events. Despite these risks, medical consensus suggests the benefits of HRT outweigh the risks. The disparity between the research and consensus means each woman should weigh the risks and benefits carefully.
Complications Associated with Hysterectomy and Oophorectomy
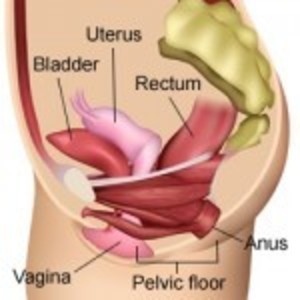
What are the risks and potential long term complications of hysterectomy, or hysterectomy plus bilateral oophorectomy? A large study of almost 30,000 nurses undergoing hysterectomy for benign (non-cancerous) diseases showed that hysterectomy plus BSO is associated with an increased risk of death from all causes, increased risk of fatal and non-fatal heart disease, and increased risk of lung cancer. Hysterectomy can cause pelvic floor dysfunction, and can negatively impact bladder function: the risks of urinary incontinence and vaginal prolapse increase significantly post-hysterectomy, although these complications usually do not develop until 10 to 20 years later.
Hysterectomy plus BSO causes surgical menopause, which causes an abrupt cessation of hormones, compared to the gradual process of natural menopause. This can result in more severe menopausal symptoms, such as hot flashes, vaginal dryness and irritation, and decreased sex drive or other problems with sexual function. In addition, the beneficial effects of the small amounts of hormones that continue to be produced post-menopause from the ovaries are gone in women who have undergone BSO. Removal of the ovaries can be devastating for some women, as observed by the personal stories shared on Hormones Matter.
Hysterectomy with or without BSO is associated with increased risk of heart disease and osteoporosis. The risk of both of these diseases increases after natural menopause, and therefore the reason the risk may increase in even in women who keep one or both ovaries at the time of hysterectomy may be partially because hysterectomy itself is associated with earlier menopause– on average by 3.7 years, when both ovaries are conserved, and by 4.4 years with unilateral oophorectomy. BSO and unilateral oophorectomy are also associated with an increased risk of Parkinson’s disease, cognitive impairment/dementia, and depression and anxiety. New research suggest the loss of hormones post oophorectomy, estradiol in particular, is detrimental to mitochondrial functioning. Mitochondrial injury is believed to be the mechanism by which post menopausal, surgically menopausal and chemically menopausal (Lupron and Lupron-like drugs) women develop a high rate of cardiovascular and neurological disease.
Things to Consider before Hysterectomy
Before a hysterectomy is considered as a treatment for recurrent pain or other endometriosis symptoms, other potential causes of pelvic pain should be considered. Pain can be from recurrent, or more likely, persistent, endometriosis, but there are many other conditions and diseases that can cause pelvic pain, such as adhesions, pelvic floor dysfunction, adenomyosis, interstitial cystitis, and nerve pain. Of these, adenomyosis is the only condition that will improve with a hysterectomy, and for some of the other conditions, a hysterectomy may cause worsening of the problems. It is a good idea to discuss all the potential causes of pelvic pain with a doctor or a team of doctors familiar with all these conditions to try to ascertain whether hysterectomy is the best potential treatment for your medical condition.
Many patients have a combination of causes contributing to their pelvic pain and other symptoms, so it can be very complicated to weigh the potential benefits against the risks. In addition, it is my opinion that given the risks and long-term complications of hysterectomy, the first line surgical treatment for endometriosis should be laparoscopic excision of all endometriosis lesions, with conservation of all reproductive organs if possible.
As someone who interacts with many endometriosis patients in my work with The Endometriosis Network Canada, patients on both sides of the hysterectomy question have told me that they feel judged for the decisions they are making or have made. I don’t believe that anyone should be judged for making the best decision they can make, taking into account their own personal situation and, preferences. However, I do want everyone making this decision to be fully armed with accurate information, so that they can make the best decision possible in what is usually a very complicated situation.




You might be interested in