The Speed of Time in Health and Disease

My father was an economist who came up with a formula for pricing derivatives called the Black-Scholes option-pricing model. He was interested in finance, but his background was physics, and his 1964 Harvard PhD thesis was about artificial intelligence. He instilled in me and my three younger sisters an abiding curiosity about the world, and a willingness to look at things in fresh ways. If I could describe him in two words, they’d be gentle irreverence.
Black-Scholes builds upon the work of others, including Louis de Broglie’s pilot-wave models, the idea of quantum equilibrium, and Brownian motion. De Broglie believed that all matter has wave properties. I am matter. Might I have wave properties, too?
In 2014, while living in a lake house in Dutchess County, New York that had a hidden mold problem, I developed a lot of issues with my health, but doctors couldn’t figure out what was wrong with me. I tried to figure out what was wrong myself, and in this essay, I will share some of what I learned with you.
Oxalate, Time, and Viral Infections
Oxalate is a crystal found in plants capable of photosynthesis. High-oxalate foods include rhubarb, tea, beets, and spinach. It can also be produced endogenously (internally). Both my parents were kidney-stone formers—most kidney stones are calcium-oxalate—and when I was sick, I seemed to do well with a low-oxalate diet.
I noticed it was when I most struggled with oxalate issues (joint inflammation, fatigue, crystals in my urine, pain at the site of old injuries) that I was most likely to experience the reactivation of old viruses. I had mononucleosis in my fourth year of college, and the Epstein-Barr virus (EBV) at times reactivates in me. Viral reactivation also occurs during spaceflight. Astronauts experience time differently than we do. Could the reason their viruses are re-activating have something to do with time?
What is time? We don’t really have a solid answer at the moment, but it is a rich area of interest and research. Some physics equations that we use to describe the universe work best if we leave time out. But, intuitively—especially since we experience time on a daily basis—leaving it out of the equation does not feel quite right.
What if it is not that time is being left out so much as that it is being compensated for? When time speeds up—light slows down. When time slows down—light speeds up. When time is too fast or too slow, light has to be too slow or too fast, respectively. When light is too slow or too fast, it is not able to appear as itself. Instead of light qua light—light as light—it will appear as … oxalate crystal?
When the Cycle Spins Backwards
Thiamine has been studied extensively by Drs. Derrick Lonsdale and Chandler Marrs, whose book, Thiamine Deficiency Disease, Dysautonomia, and High Calorie Malnutrition, explores how thiamine deficiency alters the functioning of the brainstem and autonomic nervous system by way of metabolic changes at the level of the mitochondria.
I suffered from fatigue, gastrointestinal dysfunction, joint pain, and cognitive loss. The first time I tried high-dose thiamine (vitamin B1), I had a profound recovery. My body tightened, my pain vanished, and I felt clear-headed, strong, and happy.
But, after a few weeks, I hit a wall. Thiamine lost its potency, and I stopped.
A few months later, when I tried high-dose thiamine again, I experienced something odd: a slow-motion grinding in my gut that took my breath away. For lack of a better phrase, it felt as if time were slowing down for me.
Thiamine powers the Krebs (energy) cycle. When I took it the second time around, it felt as if I had eclipsed some limit, and was powering Krebs in reverse. Instead of using my energy cycle to make energy, I was using it to make matter.
The Speed of Reality
What is the nature of reality? I was raised Catholic, and continue to love my Catholic faith. I’m inclined to respect the old sayings, such as we are the light of the world. I respect the old ideas—while also probing and questioning them.
The holographic principle was first proposed by Nobel laureate Gerard ‘t Hooft in the 1990s. In 2017, a UK, Canadian, and Italian study provided substantial evidence that the universe is, indeed, holographic. But what would that mean? I know myself—and the world—as matter, not light.
What if light functions like a plasma? A plasma is something that possesses a dual character, such as a gel. In some ways, gels behave like a liquid; in other ways, like a solid. We see a similar indeterminate quality in stem cells. A plasma’s relationship with time is that of an open gate: not limited to one direction. Neither chicken nor egg, it is a kind of chickenegg.
Perhaps light functions similarly. It can display characteristics of matter, or characteristics of energy. When time (the background fabric) is slow, light can acquire speed, like matter. When time (the background fabric) is fast, light can acquire density, like energy. At the speed of light, the perception of the background fabric flips, from “slow,” to “fast.”
[O]ur observable universe is at the threshold of expanding faster than the speed of light. ―physicist Lawrence M. Krauss
Er, “background fabric,” you say? What in the name of Michelson-Morley is that? We treat the background against which our observations are made as a vacuum—zero.
That is right. We do. I am suggesting that we may be mistaken. I am suggesting that the background here—the Cosmic Microwave Background or CMB—is not a vacuum, but matter and energy, trading places.
And that matter and energy, trading places, is light.
Like Eugene Wigner, who famously noted the unreasonable effectiveness of mathematics in describing the natural world in 1960, I am fascinated by suspiciously ubiquitous symmetry. Moon’s size: 27.27% of earth’s size. Moon’s orbital period: 27.27 days. The sun is 400 times larger than the moon—and also 400 times farther away. Hmm. Kind of makes you scratch your head a little, doesn’t it?
The black hole at the center of our galaxy, Sagittarius A*, has the largest angular size in the sky, followed by M87. M87’s black hole is 1000 times bigger, but roughly 1000 times farther away. —Feryal Özel, Harvard University Black Hole Initiative
In the spirit of Plato and René Descartes in the old age, and Nick Bostrom and Donald Hoffman in the new one, this essay asks a fundamental question: Is what we perceive an image that’s being rendered? Perhaps reality is not static, like a painting; but it has speed, like a movie.
Does it have a “correct” speed? Yes and no. It has a correct speed, but the correct speed can be achieved in different ways. It can be achieved via (for example) the color green—or via yellow + blue.
We have assumed that time is like a river whose speed we are strapped to. What if it is more like a current in which we can swim backward or forward—or tread in place? Altering the pH of my brain (e.g. with a micro dose of “acid,” LSD) seems to affect how long I am able to remain in each discrete moment of time. The more acidic, the longer—up to a point.
In other words, if we think of time as being comprised of discrete units—the way an image is pixelated, the way a movie is comprised of frames—my speed need not match time’s speed, but if it veers too far afield, I can run into problems.
Homeostasis Against the Speed of Time
I am like a glass of water, pH7. I maintain homeostasis—balance. When I perceive a background force that is expanding (high manganese?), I contract, becoming more salty. But would we perceive too much salt in the glass if the fabric against which the glass was rendered were expanding?
When I perceive a background force that’s contracting (high iron?), I expand, becoming less salty. But would we perceive too little salt in the glass if the fabric against which the glass was rendered were condensing?
Here is how time seems to operate, in me.
To one side of the baseline, time is slower (dopamine). To the other side, time is faster (serotonin).
I can slow time down, using dopamine, up to a point. But if I start to have too much dopamine, I will compensate, by hyper-methylating.
I can speed time up, using serotonin, up to a point. But if I start to have too much serotonin, I will compensate, by hypo-methylating.
This creates problems with perception. For one thing, the feeling of hypo-methylating can mimic the feeling of dopamine. Is time slow—or am *I* slow? Similarly, the feeling of hyper-methylating can mimic the feeling of serotonin. Is time fast—or am *I* fast?
What if, in Parkinson’s disease, my metronome needle is stuck all the way to the time’s left (Alpha-shifted)? I am both dopamine-toxic—and hyper-methylating.
What if, in Amyotrophic lateral sclerosis (ALS), my metronome needle is stuck all the way to time’s right (Omega-shifted)? I am both serotonin-toxic—and hypo-methylating.
In both instances, I am trapped. If I am too fast (hyper-methylating), how can I slow down if the background is too slow? But if I am too fast, the background will look too slow. If I am too slow (hypo-methylating), how can I speed up if the background is too fast? But if I’m too slow, the background will look too fast.
With two parallel trains, it is difficult to judge speed in a meaningful way. Am I slow—or is the train beside me accelerating? Am I fast—or is the train beside me decelerating?
Of Tumors and Time
I am interested in looking at the cosmos as a whole, where what we perceive (a tumor, a planet) is not fundamentally separate from its environment. This is not balls of matter in a sea of air. It is light within a speed-of-light boundary (black hole?) that is both achieving the speed of light (“sun”) and precipitating out of solution (“moon”) simultaneously. The speed of light is the 2D tipping point about which time changes directions, from acceleration to deceleration.
The perception of the speed-of-light “speed limit” depends upon an observer, and varies.
The speed of light can function like a lens. When the image becomes too dense, to one side of the lens, it becomes too expanded, on the other.
With cancer, I am deranged on both sides of time—both sides of the speed of light lens. To one side, I am too salty, too bitter. To the other, I am not salty enough. Instead of the flower, I become the fruit and the seed.
Like the speed of time, the speed of light is not necessarily a simple number (“green”); it can be a compound number (“blue + yellow”). Light has a “net” speed that I am helping to create with my own speed.
Those brown sun-spots on my shoulder? It may look as if their metronome is keeping pace with the rest of me, but what if it’s a trick of the eye? I suspect they are both denser and wider than time. They require both more magnetism (iron)—and more electricity (copper). They present as “green.” But could they be “blue and yellow, superimposed,” behind the scenes?
Once my lens curves too little or too much, I am no longer “flat” (relatively speaking); I start to have more depth than my environment. Instead of space, I start to acquire time—a new axis that is perpendicular to space the way a quasar is perpendicular to a galaxy.
What if, when I insert a new lens—a fresh perspective, “new light,” a stem cell—into an old environment, I run the risk of re-setting the metronome, and creating a new definition of so-called flatness—speed zero? Perhaps new light creates a new 2D plane from which light can expand and condense (energy)—or condense and expand (matter). It creates a “fresh green,” if you will, from which can be derived “fresh blue” and “fresh yellow.” New light is capable of operating at a different time signature—a different scale.
What does the basal cell carcinoma on my shoulder look like? A sinkpit. A small vortex. An actual indentation, like a tiny tornado. You can almost see light spinning so fast that it’s spinning backward—imploding, precipitating out of solution (rocky planets). If I use radiation or hypo-methylating agents to slow time down, I might swing too far to the other side, where light is spinning so slowly, it burns up (gas giants). Ideally, I want to be in the middle. I don’t want my metronome to be eclipsing the speed of light, to the right of time, and dipping beneath the speed of light, to the left of time, faster than the rest of my body, the rest of the universe. I want to be oscillating at the speed of light, along with the rest of the rendered world.
The Speed of Light Squared
Perhaps, in a holographic universe, the speed limit for a single universe is not the speed of light, but the speed of light squared. When we reach the speed of light squared, a new observer is created.
In this video clip, called “Microscope Imaging Station Cancer Cells behaving badly,” I believe we are witnessing cancer cells as they achieve the speed of light squared (“round up”) and become refractile. When we “round up,” we make duplicate copies of the same information (e.g. DNA). When we round up by a factor of two during embryogenesis, we produce twins. When we round up by a factor of three, we produce triplets.
We don’t create the new inside a vacuum. We make the new inside—or outside—the old.
I am interested in physicist Nikodem Poplawski’s theory that our universe is the interior of a black hole inside another universe. In fact, I wonder if we could be inside a black hole inside a black hole inside a black hole—etc.—where “black hole” is the 2D boundary known as the speed of light. Moving outward from brane to brane, scale increases. Moving inward from brane to brane, scale decreases.
A holographic universe is one in which light can serve as background or foreground, canvas or painting—or canvas and painting. As lovely as this is—are we the light of the world, for reals?—it presents difficulties with perception. How can I know what type of light I am seeing? Is what I perceive light itself, the genuine article—or light playing the role of light? Or light playing the role of light playing the role of light playing the role of light?
How many iterations of light are in an E8 crystal?
Is the speed of light functioning as a boundary we can’t see beyond? And—perhaps more importantly—is there a degree of remove above or below which light is no longer light but something else entirely—matter or energy?
The Imprecision of Time
We don’t seem to have a solid grip on time. We need leap years—even leap seconds—to make our calendars work. But there is a “cosmological constant” when it comes to time. Was there a total solar eclipse on a certain date? Add or subtract 27,729 days, and see if there was also a total solar eclipse on that date (spoiler alert: there was).
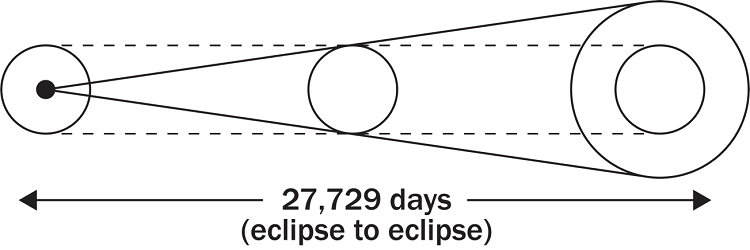
27,729 days is ~76 years, about the length of a human life. It’s also roughly 70 times 360 plus 7 times 360 days. Could it be the number of days between branes of time—the distance above or below which light undergoes a state change?
I don’t know. But here’s something interesting. The Tunguska Event took place on June 30, 1908. The largest explosion the world has ever seen, it flattened 80 million trees. No one knows what caused it. But if you add 27,729 days to the date of Tunguska, you get another date—May 31, 1984. What happened on this date?: US performs nuclear test at Nevada Test Site.
Are we living inside a singularity? Beats me; I’m a short story writer. I barely understand what a singularity is. But I do know this. I was sixteen years old in 1986. When I was a teenager, I used to love Mary Chapin Carpenter, especially a song called When Halley Came to Jackson.
“It came from the east just as bright as a torch
She saw it in the sky from her daddy’s porch
As heavenly sent as it was back then”
Funny. Halley’s Comet “comes around” every ~76 years, almost like a nuclear reaction slicing backward through the branes of time. Almost like … Chernobyl.

What if, because of the act of rendering, light can exhibit characteristics of paradox? When it eclipses the speed of light, precipitating out of solution, it’s “too cold because it’s too fast.” When it dips beneath the speed of light, burning up, it’s “too hot because it’s too slow.”
Might this type of paradox—of metabolic cul-de-sac—have bearing on human illness? If I’m “too cold because I’m too fast,” how can I slow down? I’m already too cold! If I’m “too hot because I’m too slow,” how can I speed up? I’m already too hot! Time is a veil, and I am trapped to one side.
In these models, matter, light, and energy exist on a continuum. A spectrum. Matter or energy may behave as light, in locus light, as long as allowances are made. When light is denser than light (i.e. energy), it’s too hot, but it’s able to be too hot if time is too slow (Autism?). When light is faster than light (i.e. matter), it’s too cold, but it’s able to be too cold if time is too fast (ME/CFS, Chronic Fatigue Syndrome?).
So what’s the answer? I don’t know. I’m sorry; I wish I did. I’m better at asking questions than answering them. My hope is that others who understand biology, chemistry, and physics far better than I will join the conversation, and help us to decode our illnesses.
But I do know this. When I was at my sickest, my pineal gland and my eyes did not seem to be in agreement about the character of light they were observing. Was it going fast, like matter that has speed, in a 3D image where there’s foreground and background (blue + yellow)? Or was it innately fast (green), a 2D “mono” image, where the subject itself is high-energy? The pineal gland, a tiny crystal at the center of the brain, was dubbed “the seat of the soul” by René Descartes. It sets the circadian rhythm, communicates with the HPA axis, and is the font of the neuroendocrine cascade. If hormones matter, the pineal gland matters.
The lack of an objective, outside observer is a serious constraint. How can I gauge time if the instrument I am reading time with is part of time? I have to both read time (pH) and move around in it (core metabolic rate) using the same instrument: my brain.
A Metabolic Straitjacket
After my chronic fatigue had persisted for a while, I began to realize I was wearing a metabolic straitjacket. Whatever I ate or drank was not merely providing nutrients for my body; it was providing information for my brain. This “double duty” was a huge handicap. Sodium gave me the power to increase my metabolic rate—but not the permission. Potassium gave me the permission to increase my metabolic rate—but not the power. When I would attempt a metabolic increase in spite of an acidic terrain, I would get gout-like pain. This happened a month or two before my cancer.
My basal cell carcinoma is analogous to a local high-pressure system. A planet forming in the sea of me. The cells in my shoulder are “hoarding” my time, if you will. They are stealing my electricity and my magnetism—my copper and my iron. They’ll hoard my electrolytes, too. What can I do, other than try to have them removed? If I use vasodilating agents, like raw garlic extract or niacinamide, unless I inject them, my brain reads them and responds to them, too. It does not fix the asynchrony. If I use radiation or hypo-methylating agents, to slow down time, that might work for a while, but there is a tipping point—the speed of light—above which, to slow down is actually to speed up, and these cells reach that threshold sooner than the rest of me.
It’s not that they can’t dance. They’re just dancing to a different beat.
The best thing I ever did for my health was to eliminate all glyphosate, i.e. switch to a 100% organic diet. Glyphosate (“Roundup”) was giving my brain false information about light and time. Cosmetics, underwear, mattress, etc. I will not even chew a stick of gum if it isn’t organic. Nothing makes me sicker quicker than chemical fragrance in products such as Glade plug-ins, Bounce, Downy, Tide, etc. I use organic products that treat the universe as one coherent network, a communicating whole—a garden. Because it is.
Many Worlds
I am a fan of physicist Sean Carroll and his defense of the Many Worlds interpretation of quantum mechanics, first proposed by Hugh Everett in 1957. According to Many Worlds, the universe continually splits into new branches, to produce multiple versions of ourselves. Carroll thinks that, so far, Many Worlds is the simplest possible explanation of quantum mechanics.
Many Worlds may seem exotic at first, but it possesses a simple power, especially if we treat the speed of light as a lens. When viewed from beneath the speed of light lens, light will appear to be branching into many worlds. When viewed from above the speed of light lens, light will appear to be condensing into one. At the speed of light, light is light.
If my brain misunderstands the degree of curvature of the speed of light lens, and the way the speeds of light and time titrate, it can become metabolically trapped. In Chronic Fatigue Syndrome, I may be trapped above the speed of light. Many worlds are branching faster than I am able to move through them. In Autism, I may be trapped beneath the speed of light. Many worlds are condensing faster than I am able to move through them. In Autism, it is as if I am trapped in the future. In Chronic Fatigue Syndrome, it is as if I am trapped in the past.
Endnote: Before he met my mother, my father was engaged to a brilliant woman named Frances Marshall Watkins. Fran was diagnosed with Amyotrophic Lateral Sclerosis (ALS), and died before they could wed. I would like to dedicate this essay to her. Had she not died, I would never have lived.
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, like it, please help support it. Contribute now.
Yes, I would like to support Hormones Matter.
Photo by Daniele Levis Pelusi on Unsplash.


You might be interested in

































.jpg){kind=link}