
To treat young healthy prepubescent girls with a known carcinogen to stunt their adult height sounds like a bizarre science fiction experiment, but it is unfortunately true. From 1959 through the 1970s physicians and researchers from the Royal Children’s Hospital and the University of Melbourne, gave adolescent girls of tall stature a powerful estrogenic hormone with a growing list of known side effects called diethylstilbestrol (stilboestrol) or DES.
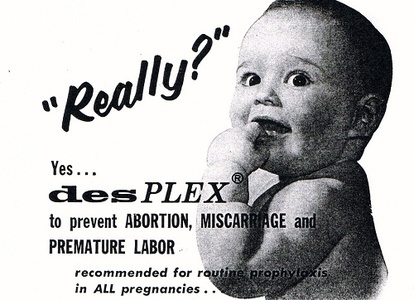
DES had been used in obstetrics to prevent miscarriage, in farm animals to bulk up livestock before slaughter, and to caponize (castrate) chickens from the 1940s through 1970s. Early on, the drug was found to be ineffective in preventing miscarriage and serious side effects including cancer were noted. Indeed, cancer in farm hands caring for animals treated with DES and concern about the effect DES-infused meat might have on human health caused the FDA to ban its use in poultry farming in 1958, well before banning its use in human women. Despite the risks associated with this drug, clinicians and researchers in Victoria Australia, funded by governmental agencies and throughout the US, Norway, and elsewhere, thought stunting the growth of tall girls, for purely psychosocial reasons, was a good idea.
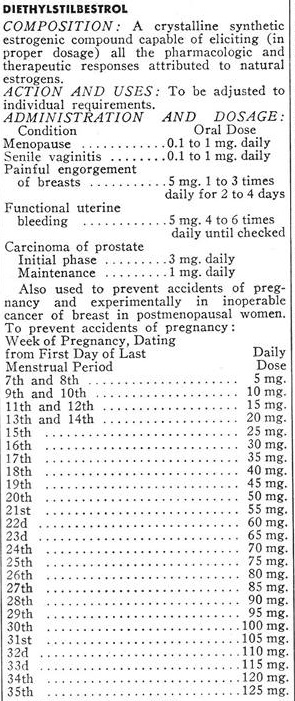
The rationale behind treating tall girls was so they could do ballet, buy clothes more easily, and find boyfriends and husbands. DES was used on healthy girls for purely psychosocial reasons. Apparently, being a tall girl was reason enough to consider medical treatment with a powerful, largely untested, synthetic estrogen with mounting evidence of carcinogenicity.
Little consideration was given to the psychosocial effects this drug would have on a young girl including nausea, the immediate onset of menstruation, the sudden development of breasts, and sudden rapid weight gain; and, of course, the long-term health outcomes of this treatment were never a consideration. The only long-term outcome considered was adult height. When meeting the tall women who underwent this treatment, it is reasonable to conclude the treatment did not work. Indeed, most of the research suggests only a 4cm reduction in height.
Discovering the Tall Girls: DES Action Australia
DES Action Australia was established in 1979 as the national support and advocacy group for individuals exposed to DES. In the early 1980s, the DES issue was new to us all and we were devouring information about its history and use. One aspect of interest was its use in veterinary practice. One of the first DES “patients” may have been Tricky Woo of the ‘All Creatures Great and Small’ books and TV series. In the late 1930s, kindly Dr. Herriot prescribed the new “wonder drug” stilboestrol for Tricky Woo’s embarrassing problem with incontinence.
Any drug which was thought to prevent miscarriage and result in bigger, healthier babies was of obvious interest to veterinary science. However, as in the earlier laboratory animal experiments, DES was soon shown to be deleterious to the health of the mother animal, to the DES-exposed offspring, and, interestingly, to subsequent litters. Thus, recommended use of DES in veterinary practice was limited to old animals and animals that were never going to breed.
We first heard of DES being used to inhibit the adult height of tall young girls almost by accident. In the early 1980s a sister of DES Action member, Clare Green, was studying veterinary science at Melbourne University. Through her, we learnt of a Melbourne veterinary scientist, Dr. Anne Jabarah, who had researched DES during the 1960s as part of her Master’s and PhD studies. Clare rang Dr. Jabarah and spoke to her at length about her research findings: that administering DES to cattle led to them subsequently developing mammary cancer. Dr. Jabarah commented that the published articles caused a great deal of interest internationally but not in Australia. Almost as an afterthought, she mentioned the Royal Children’s Hospital (RCH) here in Melbourne had requested details of her research, as they were thinking of using DES to inhibit the growth of young girls. She said she had often wondered whether they went ahead with the treatment.
Clare, on behalf of DES Action, wrote to the RCH seeking clarification on the matter. A letter was received from the medical director of the RCH stating that DES had never been used for such a purpose. In addition, Clare was asked to go into the Victorian Health Department to meet with a department spokesperson. The doctor told Clare that the matter had been looked into and there was no evidence that DES was used for this purpose. We were thus reassured, both in writing and in person, that no such trial had taken place.
So it came quite a shock several years later when I was contacted by a young woman who had been part of this nonexistent trial. She had attended the RCH and had been given DES to stunt her growth. She was in her early 20s and had been diagnosed with advanced invasive cervical cancer. As she was a nurse she knew this was very rare, particularly as she had none of the known risk factors for the disease.
When I asked her how she found out about DES Action and obtained my phone number, she said her treating doctor (a well-known Ob/Gyn) had suggested she ring. He had made the connection between her DES exposure as a young girl and the subsequent cervical cancer.
Another letter was sent to the RCH, again requesting clarification on the matter. We received back a very defensive letter in which the hospital distanced itself from the trials. They said that the clinician involved had been a private consultant and what he did in his clinics was in no way connected to the RCH.
Untangling the Tall Girls Trials after Years of Secrecy and Denials
In subsequent years (the mid-1980s to 1997) we received a handful of further inquiries from “tall girls” requesting information. Unfortunately, these were spaced too far apart for us to put the women in contact with each other. The health concerns of these women had an all-too-familiar ring: dysplasia, endometriosis, ovarian cysts, aggressive cancers (cervix and breast), impaired fertility, and premature menopause (i.e. occurring during their 20s).
I can’t really describe my feeling when I opened The Age newspaper on 27 June 1997 and read on page 1: Hormone tests on teenage girls referred to inquiry. I think the main emotion was a sense of relief – that the truth would finally be known – tall girls were given DES to stunt their growth. It also brought back to me the anger and frustration Clare and I experienced in the early 1980s when our inquiries were fobbed off by the medical establishment and health authorities.
And then my phone started ringing. As DES was mentioned in the article, the newspaper must have had me as a contact and referred any inquiries to me. Remembering how previously we were unable to put the women in contact with each other, I made a contact list of every phone call received. I explained to every caller the importance of organizing, of forming a group to share experiences, and offered to give them the list to follow up. From memory, I think Janet Cregan-Wood was about the fifth caller. She rang back the next day and “volunteered” to take on the role. And so the Tall Girls group formed and their DES story emerged.
More about DES and Tall Girls Story
- Normal at Any Cost: Tall Girls Short Boys, and the Medical Industry’s Quest to Manipulate Height
- Participation, Empowerment, and Effectiveness: The Tall Girls Inc. Experience.
- Tall Girls, Inc. Australia
- DES and the Meat Industry: My Year of Meats, by Ruth Ozeki
About the author: Marian Vickers is a DES daughter and, in 1979, was a founding member of DES Action Australia. As the DES story has evolved over the years so her focus has broadened – from issues around DES exposure to the wider issue of safety of pharmaceuticals; and finally to an understanding of endocrine disruptors and the implications for public health, particularly in terms of inadequate drug safety surveillance and reporting systems. In 2008 Marian became a ‘Gardasil mother’ when her elder daughter’s health was severely impacted by the HPV vaccine. Not only did she gain an appreciation of what DES mothers went through, she sees disturbing parallels between the DES and Gardasil stories.
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, and like it, please help support it. Contribute now.
Yes, I would like to support Hormones Matter.
This article was published originally on Hormones Matter on April 21, 2014.

You might be interested in
















 DES is not something of the past. People who have been exposed to this drug years ago are battling with health issues and fighting for their lives as I’m writing this blog post. Who knows what health problems the grandchildren of the mothers who were prescribed this drug will have to deal with as they grow up. I want my daughters to receive adequate medical care and monitoring if they ever have to suffer the consequences of this drug. This is why together with my husband we support the great work done by the very few International DES Action Groups who are providing valuable information and are advocating for the DES victims.
DES is not something of the past. People who have been exposed to this drug years ago are battling with health issues and fighting for their lives as I’m writing this blog post. Who knows what health problems the grandchildren of the mothers who were prescribed this drug will have to deal with as they grow up. I want my daughters to receive adequate medical care and monitoring if they ever have to suffer the consequences of this drug. This is why together with my husband we support the great work done by the very few International DES Action Groups who are providing valuable information and are advocating for the DES victims.




