I found a pair of slides illustrating an important scientific discovery made in 1959, which became known as the Organizational-Activational hypothesis. A team of scientists experimenting on guinea pigs, discovered that hormones early in life play a crucial role in determining the sex of the brain, and whether an animal will have male or female behavior in adult life. Similar results have since been found in numerous other animal species, and there is little doubt that the same applies to human beings too. Actually there is no doubt at all, going by my own experiences.
Basically the brain has a sex, which arises during a critical period in prenatal development (or in rats, which are born at an earlier stage of development than humans, during days 1-10 of postnatal life). If there are high levels of androgenic hormones present during this critical time, the brain becomes masculinized, and the adult behavior will be that of a male. If there aren’t androgenic hormones present, the brain develops following the default female pathway instead, and the adult behavior will be that of a female.
Rats are a particularly convenient animal for demonstrating this because their critical period occurs after birth. This makes it relatively straightforward to produce a male rat with a female brain through surgical castration at birth. With most other animals you’d have to do the surgery in utero, which is a much trickier task. It is also relatively straightforward to determine whether a particular rat has a male or female brain, because those with male brains when injected with testosterone will attempt to mate with any females present, whereas those with female brains will not. In addition, rats with female brains will adopt a posture called the lordosis posture when injected with estradiol, whereas those with male brains will not.
Organizational and Activational Effects of Hormones during Pregnancy
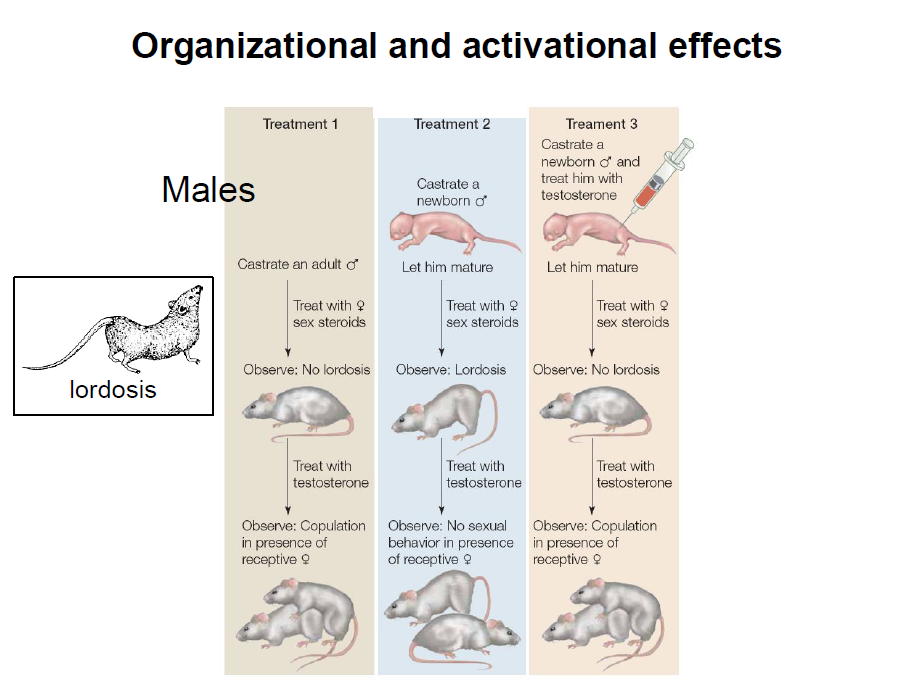
In the first graphic shown above, we see what happens to the adult behavior of males put through three different treatments:
- castrated as an adult
- castrated at birth with no supplemental testosterone
- castrated at birth, but with supplemental testosterone administered.
As is illustrated, treatments 1 and 3 result in adults that behave as males, whereas treatment 2 results in adults with female behavior. What this shows is that there is a crucial period early in the postnatal life of a rat during which either the presence of functioning testicles or externally administered testosterone causes male brain development to occur. In the absence of either, the rat ends up with a female brain, and female adult behavior despite being physically and genetically male. The period of development is roughly equivalent to gestational week 20 through birth during human pregnancy.
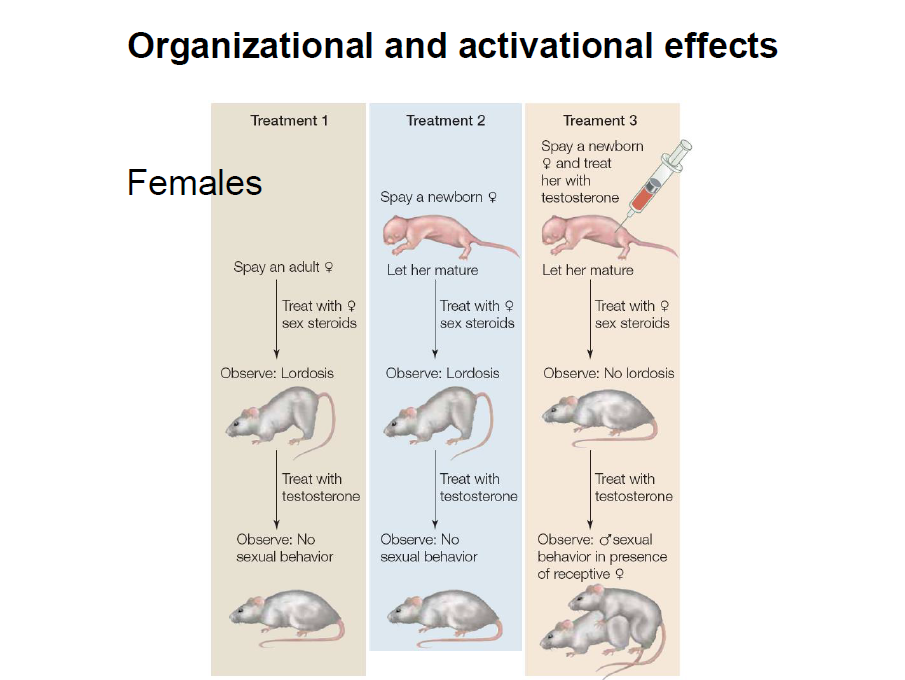
The second graphic illustrates what happens to females similarly treated. In this case through spaying, or removal of the ovaries, rather than castration. Here, only treatment 3 (spaying at birth + administering supplemental testosterone) results in an adult with male behavior. This is because, ovaries don’t produce much testosterone. So even the females spayed as adults do not have much testosterone present during the critical period for the sex of their brain. Once again, this emphasizes that it is the presence of testosterone during a critical period in brain development that produces a male brain, and the absence of that hormone during the critical period in which the brain ends up female instead. It appears that genetics and the sex of the body have nothing to do with sex based brain development. Instead, the sex of the brain is entirely dependent on whether or not androgenic hormones were present during a critical period in its development.
There are a couple of other things we can take away from this. Firstly, the effects of hormones during that critical period are permanent, and thus, are present for the remainder of the animal’s life. Secondly, anything that results in males being castrated, or females being exposed to testosterone-like hormones, during that critical period is a really bad thing, and likely to result in a male with a female brain or female with a male brain.
DES and Other Hormones Administered During Pregnancy
The miscarriage prevention drug DES given to women from the 1940s through the 1970s is a powerful chemical castration agent, so it is no small wonder that so many of the male-assigned people from DES pregnancies show signs of female brain development. The first generation progestins ethisterone and norethisterone, widely used in the 1950s and 1960s for miscarriage prevention, are both testosterone derivatives that have been shown to masculinize female fetuses (Wilkins 1960). This is why I think there’s likely to be a significant population of female assigned people from that era with male brains, as a result of their use.
DES isn’t the only drug that acts as a chemical castration agent to have been used during pregnancy. Progestins can also act as chemical castration agents, and unlike DES, they were never withdrawn, but remain in use even now. The archetypal progestin, medroxyprogesterone acetate (MPA), is one of the most popular drugs for chemical castration of sex offenders. It is in my 1972 Monthly Index of Medical Specialties (MIMS) and 1981 British National Formulary for treatment of habitual abortion (i.e. miscarriage prevention), so has definitely been used in human pregnancies in the past.
More to the point, hydroxyprogesterone caproate, which seems to be the most popular currently used miscarriage preventative, has similar pharmacological properties to MPA. The primary difference is that it is a pure progestin that doesn’t cross-react with non-target receptor types, whereas MPA, to a small extent, does. Other than that, they are quite similar drugs with similar effects. Therefore, I think there is a big risk of male assigned children from pregnancies in which hydroxyprogesterone caproate is used, being born with female brains. It is certainly something that bears looking at, by people independent of the pharmaceutical industry and the medical establishment.
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, like it, please help support it. Contribute now.
Yes, I would like to support Hormones Matter.
Feature image credit: desktop wallpapers.
This article was published originally in July 2019.



You might be interested in













 DES is not something of the past. People who have been exposed to this drug years ago are battling with health issues and fighting for their lives as I’m writing this blog post. Who knows what health problems the grandchildren of the mothers who were prescribed this drug will have to deal with as they grow up. I want my daughters to receive adequate medical care and monitoring if they ever have to suffer the consequences of this drug. This is why together with my husband we support the great work done by the very few International DES Action Groups who are providing valuable information and are advocating for the DES victims.
DES is not something of the past. People who have been exposed to this drug years ago are battling with health issues and fighting for their lives as I’m writing this blog post. Who knows what health problems the grandchildren of the mothers who were prescribed this drug will have to deal with as they grow up. I want my daughters to receive adequate medical care and monitoring if they ever have to suffer the consequences of this drug. This is why together with my husband we support the great work done by the very few International DES Action Groups who are providing valuable information and are advocating for the DES victims.