Have you noticed how the nutritional world is changing all around you? Latest news on television: the drop in sugar consumption placed manufacturers at a tipping point of collapse. News a few weeks earlier: grocery stores are redesigning their stores and the products they carry because the middle aisles are not used by shoppers (that is where they usually keep cereals, grains, sugars, and canned or boxed processed foods, cooking oils). McDonald’s announced not too many months ago that they are dropping high fructose corn syrup from their buns and several other fast food chains advertise wholesome fresh foods without sugar. Restaurants are popping up where glutinous grains are not served.
The interesting commonality about all of this is that these are all anecdotal evidences that the scientific world refuses to notice. What will it take scientists to become curious? A change in funding sources for research perhaps?
No one is suggesting that anecdotal evidence is science. It is not. Anecdotal evidence is defined as follows:
“Anecdotal evidence is evidence from anecdotes, i.e., evidence collected in a casual or informal manner and relying heavily or entirely on personal testimony. … Thus, even when accurate, anecdotal evidence is not necessarily representative of a typical experience.” (Wikipedia)
By definition, scientific “evidence” doesn’t exist. So, we must use the scientific method’s definition:
“A systematic approach to solving a problem by discovering knowledge, investigating a phenomenon, verifying and integrating previous knowledge. It follows a series of steps that evaluates the veracity or the feasibility of a prediction through research and experimentation from where the information obtained will be used as a basis in making conclusions.
The fundamental steps of scientific method are:
(1) Identifying the problem to solve
(2) Formulating a tentative answer or hypothesis
(3) Testing the hypothesis
(4) Gathering and analyzing data
(5) Making conclusions” (from the biology online dictionary)”
Looking at it this way, the only way scientific examination can yield any results that can be interpreted in usefulness (or lack thereof) and officially applied to a population is by experimenting in a controlled environment, testing every possible outcome, and finding what does or does not work, and most importantly: find out why and/or how.
The Evidence for Diet: Anecdotal or Scientific?
One of the most studied databases for scientific research is the Women’s Health Initiative (WHI), which is an ongoing study of over 80 years. As you can see at this link, the data has been collected three ways: self-administered forms, interviews, and clinical measurements, such as a general physical exam. You can see here the data collection methods. There is absolutely no scientific method whatsoever in this study. The only difference between this study and a survey posted anywhere on the internet about what people eat, is who does the asking, the data collection, and where the funding comes from.
Another famous dataset that researchers constantly analyze is the National Health and Nutrition Examination Survey, the NHANES dataset. This too is based on surveys and questionnaires. The questionnaires for 2015 are found here. There is no scientific method applied in them whatsoever.
However, both the WHI and the NHANES have been treated as the gold standard for scientific evaluation to the degree of making health and nutrition regulation for the US over the past nearly 60+ years. The nutrition guideline (even the latest one created in 2015), the heart-health movement, high cholesterol treatment with the statin ideology, the low fat hypothesis by Ancel Keys, and several other nutritional and medical decisions, including reduced salt intake requirement for hypertension, originally called the Rice Diet founded by Walter Kemper, had all been made based on datasets like these. Note that these datasets are all just anecdotal evidence. They twisted our imagination into believing that they are science because of the funding source (often National Institutes of Health, the NIH), the scope, and the length of the data collection.
While there is no science in data collection, so much of our lives have been changed (often destroyed) by the regulations made based on the often-faulty statistical analysis of these datasets that it is scary. The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) tells us that 2 out of 3 (67%) Americans are overweight or obese and 1 in 3 (33%) are obese. In 2014 (the latest statistics available), over 9% of the population had diabetes. In 2015, a JAMA report suggested that over 50% of the US population was either pre-diabetic or had diabetes by 2012. This is scary indeed!
Although the cause of these very sad changes are highly debated and controversial, it is important to note a very strong point: the start of the deteriorating health of the US population coincides with the nutrition and health regulations brought about as a result of these two and several other similar databases. Note that thee databases are collections of anecdotal evidence that masquerade as scientific evidence—they are not. There has never been any shred of scientific evidence that a high carbohydrate diet is healthier than a low carbohydrate diet, yet current nutritional guidelines suggest that there is such evidence. There isn’t any. There are many research papers published based on the assumption that these guidelines are correct, in which the researchers tried to prove that they are correct. However, in science, one cannot prove something correct. The role of science is to try to disprove by replication and finding mistakes and if all attempts at disproving fail, perhaps the findings stand. There is not a single research paper published according to these guidelines based on the above noted datasets.
The Diet Underground
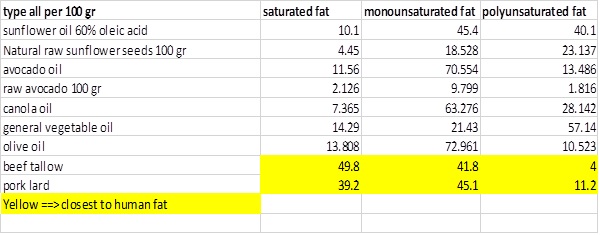
While scientists argue and face-off in debates of trying to make each other look bad, there is a different movement taking place that is apparently unnoticed by scientists: it is an underground grassroots movement of people changing their dietary habits and shaking obesity, insulin resistance, type 2 diabetes, non-alcoholic fatty liver disease, hypertension, and all kinds of other health conditions. And they are doing it all by self-initiated dietary changes—not with the help of nutritional experts or doctors and definitely not with any medicines. It is because of this underground movement that grocery stores are now reevaluating the products they carry, why McDonald’s and other fast food chains dropped HFCS, and why people are stopping the consumption of vegetable oils and cook with animal fats instead.
Anecdotal evidence is piling up in favor of the health benefits of the “modern human” who no longer eats grains or sugar and who cooks with animal fats.
Social Media and the Rise of Anecdotal Evidence
I counted the number of weight loss groups on Facebook. There are over 500. At least five of these groups have over 20,000 members, so that is over 100,000 people. Ketogenic groups are much larger; many have over 70,000 members and one had almost 400,000 members. There are more ketogenic groups on Facebook than weight loss groups—I could never reach the end of the list after five minutes of scrolling so I gave up. I estimate the number of people in ketogenic groups to be over one million. Although the Atkins Diet is the original ketogenic diet, since few people realize that, there are about 100 Atkins Diet groups, with one boasting nearly 400,000 members and several over 10,000 so I estimate about 500,000 people on the Atkins Diet just on Facebook. Similarly, there are about 300 low carbs high fat (LCHF) groups of Facebook with several groups over 10 thousand in membership, one close to 40,000 so I estimate approximately 100,000 members in the LCHF groups.
If you visit any of these groups, you will find amazing success stories of weight loss, reversal of type 2 diabetes, pre-diabetes, insulin resistance, non-alcoholic fatty liver disease, allergies, arthritis, asthma, etc. In total, I just noted ~2 million people (granted some people may be in many groups but as a rough estimate) as anecdotal evidence (just on Facebook alone) who have proven (to themselves and to scientists who wish to listen) everything that flies in the face of nutrition and medicine guidelines currently enforced and practiced. Since scientists dismiss the movement as a fad, few scientists like me participate in observation, let alone practicing this “fad” to see if it really is better than the official guidelines-driven nutrition and healthcare.
As a scientist myself, I do participate actively in some of these Facebook groups, and even have several of my own, in which members practice these so called “fads” and indeed are shedding weight, healing from migraines, diabetes, insulin resistance, hypertension, etc. A scientist may now say that “but these are only placebo effects.” That is very hard to envision since these people also stop all their medicines, all of which came through clinical trials tested for efficacy against placebo. Increating to weight 400 lbs over the years on the officially supported nutritional guidelines in spite of all efforts to get rid of the weight, and then losing it all in a year by a nutritional change and becoming healthier at the same time, speaks volumes!! And I see this happen over and over again!
I often hear that “oh but this is just short term.” I have yet to have any scientist define what “short term” versus “long term” means in their experimental mode but someone who has been on a changed nutritional diet for over two years (me) is definitely not short term. There are many people who have been following these new nutritional paradigms for over 10, 15, and some 20 years. Is that really short term?
The Winners
The ultimate decision is not in the hands of the scientists, the nutritional experts, or the healthcare providers. The judgment of what people will do is in the hands of the people. It seems, just by sheer numbers and success stories, that science is losing out big time. Instead of opening their minds and evaluating why and how these nutritional changes work, most scientists stay closed off in their dogmatic corners. There are a few scientists who try to publish their findings of the benefits of the “fad” nutrition but they seldom get published because the publishers are members of the dogmatic team. In reality though, none of that matters. What matters is information exchange and the changing markets as a result of pressure by the majority who want out from under the dogma umbrella. One way or another the new and healthy will win. Whether you join or are left behind is only up to you.
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, like it, please help support it. Contribute now.
Yes, I would like to support Hormones Matter.
This article was published originally on June 5, 2017.




You might be interested in