Before I get further into dissecting the Nelson Pill Hearings I want to pause and talk about feminism and my intent for this project. The history of the birth control pill and the history of feminism are closely tied, because, of course, if women can control when and/or whether they have children, they have power over their own lives. First-wave feminists knew this. It was Margaret Sanger after all who coined the term “birth control” and conceived (pardon the pun) the idea of the pill in the first place. And so it’s no surprise that the release of the birth control pill in 1960 ushered in the second wave of feminism.
Somewhere, somehow, many people confused the right to choose with blind acceptance of hormonal birth control as “freedom.” These may be the same people who liken questioning the government with being unpatriotic. I suggest that in a democracy it is our most patriotic duty to scrutinize whether our government is acting in the best interest of its people. Likewise, as feminists it is our duty to scrutinize what may or may not be serving women.
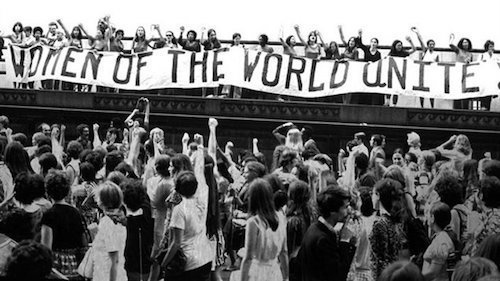
The F Words – Feminism and Freedom
Many people believe that having unlimited access to every kind of birth control is the only way to be a feminist and therefore speaking out against the pill or other hormonal birth control is anti-women. Let us consider for a moment the types of birth control that are encouraged, advertised, and prescribed, and with these medications, whose body is being affected? Who will pay if these methods fail? Who has to deal with the side effects? As someone who suffered a stroke while on the birth control pill, I am keenly aware of the price that comes with this “freedom.”
Anti-feminists like to write a lot of articles about how women want to have it all—as if everyone doesn’t want to have it all. That’s not a feminist concept, that’s an American ideal. So, yes, as an American I want to have it all. I want birth control that doesn’t come with the risk of blood clots. I want birth control that isn’t going to kill me, make me fat, give me acne, create mood swings, or lower my libido. Why would I want all the freedom to have sex without getting pregnant with none of the desire to actually have sex?
Why is Birth Control the Sole Responsibility of Women?
Which brings us to the question—where is the pill for men? Still being tested? We hear about this birth control for men every few years, but it has yet to materialize. Is that because it’s being more thoroughly tested than any hormonal birth control they have ever released for women? The original birth control pill was tested on poor women in Puerto Rico who were not even informed that they were part of a study. This article cannot even begin to explore how the fertility of poor and minority women has been systematically targeted and abused in the name of limiting population growth. That’s a whole other topic. And I’ll be explaining the Puerto Rican trials more in future articles but it is important to note that there were only two years between when the research in Puerto Rico began and the birth control pill was approved for use in the United States. Yet every article about birth control for men suggests that many more years of study are required before we’ll every see this as a reality.
But maybe there is no pill for men yet because the side effects have been deemed unacceptable?
At the Nelson Pill Hearings, Dr. Whitelaw, a private physician and early fertility specialist, asked, “How many adult males would be willing to take an oral contraceptive faithfully if they were told that instead of a possible 50-plus adverse side reaction only one remained, that being the possible loss of sex drive and libido?” How many indeed.
But if loss of libido doesn’t scare you, how about the “50-plus adverse side reactions”? Even in 1970, hormonal birth control was linked not just to blood clots (and by extension DVT, PE, and stroke) but also to cancer, infertility, miscarriages, and even diabetes and rheumatoid arthritis. And that’s just the beginning.
However, and this is a big HOWEVER- it is not my goal to demonize the pill or any other hormonal birth control. It is not my goal to unnecessarily scare people. It’s simply my goal to educate about the dangers of these hormones that are over-prescribed and under-researched. Because I’m a feminist, I believe it is a woman’s right to choose. But that choice must be an informed one. Soon I’ll be writing more about how women are informed by looking at risk communication with these and other medicines.
Information or Patronization?
From what I’ve read so far in the hearings, every doctor who has testified has agreed that women need to be better informed of the dangers of hormonal birth control. Except one. Dr. Robert W. Kistner from the Department of Obstetrics and Gynecology Harvard Medical School said, “I don’t believe it is good medical practice with any medication to go through the list of possible complications.” And by way of explanation for this he says that if you tell a woman that headaches are a possible side effect of the birth control pill, then they will get headaches. I wonder if the same can be said for blood clots? It is also interesting to note when Dr. Kistner was asked by the committee if he had ever worked for the pharmaceutical companies, he answered, “Yes, all of them.”
Maybe it’s time for people like Dr. Kistner and Senator Bob Dole, who was also at the Nelson Pill Hearings, to stop being concerned with women’s “emotional reactions” to information about the pill. And give us the full story even though he thinks it may “confuse the women we seek to protect.” Because unlike Bob Dole, I think that women not only can handle the truth about hormonal birth control, but that they deserve it. It’s time to stop allowing corporations and agenda-driven legislation to decide what we can and cannot understand, what we do and don’t need to know about medications that affect us.
Because are women really liberated if we have taken the freedom to choose and handed it to pharmaceutical companies?
Real Risk Study: Birth Control and Blood Clots
Lucine Health Sciences and Hormones Matter are conducting research to investigate the relationship between hormonal birth control and blood clots. If you or a loved one have suffered from a blood clot while using hormonal birth control, please consider participating. We are also looking for participants who have been using hormonal birth control for at least one year and have NOT had a blood clot, as well as women who have NEVER used hormonal birth control. For more information or to participate, click here.
Related posts:

You might be interested in