Topamax: The Drug with 9 Lives
Is Topamax a Wonder Drug?
Over the past week alone, I have talked to several people about their doctor visits. Each one of them had a different illness and each one of them was prescribed the drug Topamax. I cannot help but wondering, how it is possible that one medication can treat so many disparate illnesses. I suspect it cannot and the overreach is driven more by marketing than medicine. This led me to do some digging into Topamax.
What I found is not good. Topamax is prescribed for a broad scope of illnesses for which there is likely little evidence of its efficacy. Take a look at the list below.
Illnesses or Conditions for which Topamax is Prescribed
- Obesity1. Medicine: Topamax
- Seizures1. Medicine: Topamax
- Migraine1,2. Medicine: Topamax
- Impulsivity3. Medicine: Topamax
- Diabetes with nerve damage4. Medicine: Topamax
- Bipolar disorder5. Medicine: Topamax
- Depression6. Medicine: Topamax
- Alcohol addiction7: Topamax
- Fibromyalgia8. Medicine: Topamax
I would like to add a 10th to that: I have broken a nail…can I get Topamax?
Honestly, off-label prescribing has gone too far! Does Topamax really treat so many disparate conditions that doctors prescribe it for everything, even when it is not FDA approved for these conditions? I must add that Topamax is one of the most dangerous drugs in the prescription market today. Not only is it a diet pill made from sugar derivatives (actually a sugar substitute) but it uses two dangerous methods (blocking both voltage dependent calcium and voltage gated sodium channels at once) to achieve what several classes of drugs normally do separately; and thus, with one medicine it affects and potentially damages the two circuits that are critical for brain function. Topamax (an anticonvulsant under additional name Topiramate (generic) and in time release Trokendi XR) is important to discuss because it was initially formulated as a diet pill. Yet over 50% of the new members who join my migraine group arrive with Topamax on their prescription list.
I have yet to find a single person on this drug who is not seriously considering dropping it due to its adverse effects, not to mention that it does not appear to work as a pain killer. Unfortunately, Topamax is difficult to quit. The most difficult problem is that doctors are under the false impression that a drug that blocks the voltage dependent calcium and potassium channels can just be easily stopped by a few days of reduction. However, since the voltage dependent calcium channel is a high voltage channel, for some people the discontinuation may end in seizures.
Evidence is also accumulating that Topamax can cause brain damage 4. Personally, I have heard of many cases where it in fact has done just that.
Topamax is a sugar substitute that failed as a diet pill but is somehow permitted by the FDA to be used for epileptic seizures. It also received approval for use against migraines. The reasons for such a turn of events is unclear; how can a drug that fails approval for a diet pill suddenly be a perfect match for seizures and migraines? Don’t we all wish for sugar pill to be a pain killer? Unfortunately, sugar or sugar substitutes do not have such serious adverse effects as Topamax (they happen to have different ones).
Adverse effects of Topamax
If we look at the list of adverse effects associated with this drug (as provided by Wikipedia – Topamax), it is clear that Topamax is not very safe. Indeed, the list is very long.
Dizziness, Weight loss, Paraesthesia (pins and needles), Somnolence, Nausea, Diarrhea, Fatigue, Nasopharyngitis – common cold, Depression, Weight gain, Anaemia, Disturbance in attention, Memory impairment, Amnesia, Cognitive disorder, Mental impairment, Psychomotor skills impaired, Convulsion, Coordination abnormal, Tremor, Lethargy, Hypoaesthesia, Nystagmus, Dysgeusia, Balance disorder, Dysarthria, Intention tremor, Sedation, Vision blurred, Diplopia, Visual disturbance, Vertigo, Tinnitus, Ear pain, Dyspnoea, Epistaxis, Nasal congestion, Rhinorrhoea, Vomiting, Constipation, Abdominal pain, Dyspepsia, Dry mouth, Stomach discomfort, Paraesthesia oral, Gastritis, Abdominal discomfort, Nephrolithiasis, Pollakisuria, Dysuria, Alopecia (hair loss), Rash, Pruritus, Arthralgia, Muscle spasms, Myalgia, Muscle twitching, Muscular weakness, Musculoskeletal chest pain, Anorexia, Decreased appetite, Pyrexia, Asthenia, Irritability, Gait disturbance, Feeling abnormal, Malaise, Hypersensitivity, Bradyphrenia, Insomnia, Expressive language disorder, Anxiety, Confusional state, Disorientation, Aggression, Mood altered, Agitation, Mood swings, Anger, Abnormal behavior, Crystal urine present, Tandem gait test abnormal, White blood cell count decreased, Bradycardia, Sinus bradycardia, Palpitations, Leucopenia, Thrombocytopenia, Lymphadenopathy, Eosinophilia, Depressed level of consciousness, Grand mal convulsion, Visual field defect, Complex partial seizures, Speech disorder, Psychomotor hyperactivity, Syncope, sensory disturbance, Drooling, Hypersomnia, Aphasia, Repetitive speech (stuttering), Hypokinesia, Dyskinesia, Dizziness postural, Poor quality sleep, Burning sensation, Sensory loss, Parosmia, Cerebellar syndrome, Dysaesthesia, Hypogeusia, Stupor, Clumsiness, Aura, Ageusia, Dysgraphia, Dysphasia, Neuropathy peripheral, Presyncope, Dystonia, Formication (the sensation of insects crawling under the skin), Visual acuity reduced, Scotoma, Myopia, Abnormal sensation in eye, Dry eye, Photophobia, Blepharospasm, Lacrimation increased, Photopsia, Mydriasis, Presbyopia, Deafness, Deafness unilateral, Deafness neurosensory, Ear discomfort, Hearing impaired, Dyspnoea exertional, Paranasal sinus hypersecretion, Dysphonia, Pancreatitis, Flatulence, Gastrooesophageal reflux disease, Hypoaesthesia oral gingival bleeding, Abdominal distension, Epigastric discomfort, Abdominal tenderness, Salivary hypersecretion, Oral pain, Breath odour, Glossodynia, Calculus urinary, Urinary incontinence, Haematuria (blood in urine), Incontinence, Micturition urgency, Renal colic, Renal pain, Anhidrosis, Hypoaesthesia facial, Urticaria, Erythema, Pruritus generalized, Rash macular, Skin discolouration, Allergic dermatitis, Swelling face, Joint swelling, Musculoskeletal stiffness, Flank pain, Muscle fatigue, Metabolic acidosis, Hypokalaemia, Increased appetite, Polydipsia, Hypotension, Orthostatic hypotension flushing, Hot flush, Hyperthermia, Thirst, Influenza like illness, Sluggishness, Peripheral coldness, Feeling drunk, Feeling jittery, Learning disability, Erectile dysfunction, Sexual dysfunction, Suicidal ideation, Suicide attempt, Hallucination, Psychotic disorder, Apathy, Lack of spontaneous speech, Sleep disorder, Affect lability, Libido decreased, Restlessness, Crying, Dysphemia, Euphoric mood, Paranoia, Perseveration, Panic attack, Tearfulness, Reading disorder, Initial insomnia, Flat affect, Thinking abnormal, Loss of libido, Listless, Middle insomnia, Distractibility, Early morning awakening, Panic reaction, Elevated mood, Blood bicarbonate decreased, Neutropaenia, Apraxia, Circadian rhythm sleep disorder, Hyperaesthesia, Hyposmia, Anosmia, Essential tremor, Akinesia, Unresponsive to stimuli, Blindness unilateral, Blindness transient, Glaucoma, Accommodation disorder, Altered visual depth perception, Scintillating scotoma, Eyelid edema, Night blindness, Amblyopia, Calculus ureteric, Renal tubular acidosis, Stevens-Johnson syndrome, Erythema multiforme, Skin odour abnormal, Periorbital oedema, Urticaria localized, Limb discomfort, Acidosis hyperchloraemic, Raynaud’s phenomenon, Face edema, Calcinosis, Mania, Anorgasmia, Panic disorder, Disturbance in sexual arousal, Feeling of despair, Orgasm abnormal, Hypomania, Orgasmic sensation decreased.
The FDA Black Box on Topamax
According to the FDA and their listed label update in 2014, Topomax includes a black-box warning that has the following known adverse effects:
- Acute myopia and secondary angle closure glaucoma: Untreated elevated intraocular pressure can lead to permanent visual loss. The primary treatment to reverse symptoms is discontinuation of TOPAMAX as rapidly as possible (5.1)
- Visual field defects: These have been reported independent of elevated intraocular pressure. Consider discontinuation of TOPAMAX (5.2)
- Oligohidrosis and hyperthermia: Monitor decreased sweating and increased body temperature, especially in pediatric patients (5.3)
- Metabolic acidosis: Baseline and periodic measurement of serum bicarbonate is recommended. Consider dose reduction or discontinuation of TOPAMAX if clinically appropriate (5.4)
- Suicidal behavior and ideation: Antiepileptic drugs increase the risk of suicidal behavior or ideation (5.5)
- Cognitive/neuropsychiatric: TOPAMAX may cause cognitive dysfunction. Patients should use caution when operating machinery including automobiles. Depression and mood problems may occur in epilepsy and migraine populations (5.6)
- Fetal Toxicity: TOPAMAX use during pregnancy can cause cleft lip and/or palate (5.7)
- Withdrawal of AEDs: Withdrawal of TOPAMAX should be done gradually (5.8)
- Hyperammonemia and encephalopathy associated with or without concomitant valproic acid use: Patients with inborn errors of metabolism or reduced mitochondrial activity may have an increased risk of hyperammonemia. Measure ammonia if encephalopathic symptoms occur (5.10)
- Kidney stones: Use with other carbonic anhydrase inhibitors, other drugs causing metabolic acidosis, or in patients on a ketogenic diet should be avoided (5.11)
- Hypothermia has been reported with and without hyperammonemia during topiramate treatment with concomitant valproic acid use (5.12) (FDA Topamax Label)
According to the label, Topamax is only indicated for seizures as a secondary medication in support of a primary kind and for migraines and nothing else (not even for diet anymore). Yet, I see people being prescribed this drug for all types of off-label use that are unrelated to either seizures or migraines. The large migraine group I run on Facebook grown to over 4000 migraineurs in the past two years.
Because I have found that Topamax is the #1 prescribed medicine to migraineurs when they join the group in despair and hopelessness, I have decided to designate Topamax also as the #1 medicine discussed on the series titled drugs of shame. This is apt because it affects (and often damages) the neurotransmitters (hormones of the brain) and thereby puts the whole hormonal structure of the body in chaos.
The Problem: Brain Slowing
Topamax may cause brain function slowing. Why? Topamax is a voltage dependent calcium channel blocker (also called voltage-gated calcium channel blocker), which is a key channel for neuron communication via neurotransmitter release. Topamax is systemic, meaning it doesn’t just act on a particular type of neurons but all neurons. This means that neurons that are responsible to organize how the heart beats, how the lungs function, how you blink, and how you digest are all affected by Topamax in a negative way: the neurons cannot release neurotransmitters and so the communication between hormones of the brain and the hormones of the body are broken. Many of the side effects of Topamax are so strong that migraineurs who start Topamax stop within weeks (some on day 3) of initiating this medication. The drawing below shows how voltage dependent calcium channels work and what happens when they cannot work because they are blocked.
Voltage Dependent Calcium Channel Blockers
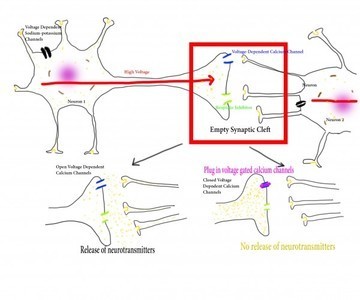
Figure 1. How Voltage Dependent Calcium Channels Work
In figure 1 you see a simplified neuron on the left and the axons of another neuron on the right. In the synaptic cleft normally neurotransmitters work like a domino effect. One neuron receives a signal from a sensory organ that stimulates the release of neurotransmitters that are specific to the type of stimulus. The neurotransmitters then get to be picked up by the neuron connected to the releasing neuron and pass the signal along. When the signal volume, intensity, frequency reaches a particular threshold, the brain sends a command to the body: wipe nose, for example.
Blocking the voltage dependent calcium channels from firing means that no neurotransmitters can be released and thus no message is passed on to the necessary number of neurons to reach the threshold. Since Topamax is systemic, every function of the body is hampered to some degree.
Neurons have five types of voltage dependent calcium channels based on voltage requirements:
- L-type that directs skeletal muscles, cardiac related muscle cells, endocrine cells, adrenal, etc., associated with contraction, hormone release and synaptic integration (neurons working together)
- P/Q-type that activate neurons and neurotransmitter and hormone release
- N-type works at the nerve terminals similarly to P/Q for neurotransmitter and hormone release
- T-type think of it as the pacemaker of the brain for firing with a particular frequency
- R-type that works with cerebral cells and some neurons
For each of these, the current required is different so fine-tuning is necessary. The calcium channel must go through all stages of voltage levels to be able to perform all five types of actions, as the body requires all of them. Note that when the voltage gated calcium channels are blocked, none of these 5 types of actions can properly function. The body will utilize its reserves to maintain vital functions. People who take Topamax can still breathe and their hearts beat – but they have serious issues, for example, with body cooling, which is a pretty basic, built-in automatic motor function. People who take Topamax overheat and cannot cool themselves. Most interestingly Topamax prevents the very functions a migraine brain needs for relief the most because it blocks those channels that would instruct the brain to cool the body.
In addition, Topamax blocks both voltage dependent sodium-potassium channels. I have written extensively on voltage dependent sodium-potassium channels in previous articles so here I just present a short summary. Voltage dependent (or gated) sodium-potassium channels have the critical function of sodium and potassium exchange in the cell to ensure that proper voltage is created in the cell membrane. Proper voltage is required so that the channels can open and close their gates, nutrients can enter and waste products can leave. Neurons cannot manufacture neurotransmitters without the availability of various minerals, many of which must be able to enter the neuron via voltage gated sodium-potassium channels. When these channels are not able to generate the proper action potential, nothing moves in or out of the neuron. By blocking voltage dependent channels, the high voltage needed to release the neurotransmitters is dulled as well.
Topamax robs the brain from its most important vital roles: making neurotransmitters that transmit messages and regulate brain and important autonomic body functions such as, cooling the body when it is too hot, maintaining and appropriate heart beat, or simply making a decision1. I think, Topamax is one of the more dangerous drugs on the market. From what I can gather from the research and my work with migraineurs, Topamax does not appear to work for pain. It only slows brain function. I would not be surprised to see researchers soon showing a connection between Topamax use and dementia. Until then, proceed with caution.
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, like it, please help support it. Contribute now.
Yes, I would like to support Hormones Matter.
Sources
1 Sommer, B. R., Mitchell, E. L. & Wroolie, T. E. Topiramate: Effects on cognition in patients with epilepsy, migraine headache and obesity. Therapeutic Advances in Neurological Disorders 6, 211-227, doi:10.1177/1756285613481257 (2013).
2 Nelles, G. et al. Prevention of episodic migraines with topiramate: results from a non-interventional study in a general practice setting. The Journal of Headache and Pain 11, 33-44, doi:10.1007/s10194-009-0163-x (2010).
3 Navarrete, F., Pérez-Ortiz, J. M. & Manzanares, J. Pregabalin- and topiramate-mediated regulation of cognitive and motor impulsivity in DBA/2 mice. British Journal of Pharmacology 167, 183-195, doi:10.1111/j.1476-5381.2012.01981.x (2012).
4 Garvey, W. T. Phentermine and topiramate extended-release: a new treatment for obesity and its role in a complications-centric approach to obesity medical management. Expert Opinion on Drug Safety 12, 741-756, doi:10.1517/14740338.2013.806481 (2013).
5 Geddes, J. R. & Miklowitz, D. J. Treatment of bipolar disorder. Lancet 381, 10.1016/S0140-6736(1013)60857-60850, doi:10.1016/S0140-6736(13)60857-0 (2013).
6 Campayo, J. G. et al. Effectiveness of topiramate for tobacco dependence in patients with depression; a randomised, controlled trial. BMC Family Practice 9, 28-28, doi:10.1186/1471-2296-9-28 (2008).
7 Johnson, B. A. & Ait-Daoud, N. Topiramate in the New Generations of Drugs: Efficacy in the Treatment of Alcoholic Patients. Current pharmaceutical design 16, 2103-2112 (2010).
8 Pereira, A. G., Michael J.; Gross, Robert A.; Posner, Kelly; Dworkin, Robert H. Suicidality associated with anti-epileptic drugs: implications for the treatment of neuropathic pain and fibromyalgia. Pain 154, 345-349 (2013).
This article was first published on September 10, 2015.



You might be interested in





