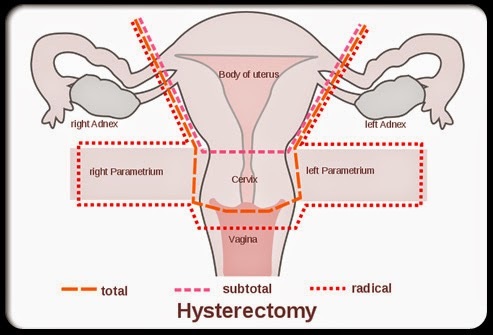
Hysterectomy Experiences: Chronic Fatigue

A few years ago, I began writing for Hormones Matter about the gross overuse and adverse effects of hysterectomy and oophorectomy. Year after year, these posts generate tens of thousands of views and hundreds of comments. The comments inevitably follow the same pattern of unwarranted removal of organ(s) without informed consent and ensuing declining health. We are publishing a series of articles highlighting women’s comments. This is the fifth of the series and addresses the common complaint of chronic fatigue. The first article is about lack of informed consent and can be found here. The second one talks about how our “exterior” settles / collapses after the uterus is removed. The third addresses organ dysfunction and the fourth is about loss of sexuality and emotional emptiness. Although the 90% elective rate of these surgeries would imply that they are “restorative” or at least harmless, medical literature and women’s experiences prove otherwise.
Chronic Fatigue and Loss of Stamina
Many women commented on my other articles about chronic fatigue and loss of stamina and vibrancy since their hysterectomies even if they still had their ovaries. Although sleep problems were a common complaint, even absent those, women just couldn’t seem to get past the chronic fatigue and lack of stamina. These experiences match those of the majority of 1,000 hysterectomized women surveyed by the non-profit HERS Foundation. Those results are as follows:
- Loss of energy: 78%
- Profound fatigue: 77%
- Loss of stamina: 69%
- Insomnia: 61%
- Unable to maintain previous level of activity in home: 34%
The complete list broken out by hysterectomy only, hysterectomy with one ovary removed, and hysterectomy with both ovaries removed can be found here. Below are comments from some of my articles.
Chris (age 64) says:
“My husband and I had and unbelievable sex life, I had loads of energy and strength and was able to joke about being “37”. I now feel like and old woman. I want to sleep more then move, I have little strength….”
Jacqueline:
“I have no energy at 38. I have more problems now than I did before surgery.”
NJ:
“The Testim has helped my energy levels but I have lowered the dose as my body hair increased.”
Joshua:
“…my finance had a cervical hysterectomy [sic] back in January of this year and she seems to be having issues with mood swings sex drive depression and fatigue.”
BeBe:
“My hysterectomy was necessary due to Essure permanent birth control. One migrated to my uterus and I was sick from that poison…. I’m 11 months post op…. I’m fatigued. Have migraines and have become very anti social.”
Joan:
“I was a very active women, always running around from 6am till 9pm…. I am tired all the time.”
Teresa:
“I’m 12 years post op…. I stay fatigued and have no sexual drive and depression….”
Sue:
“Hysterectomy [sic] in 2007…. Severe fatigue, bloating, pain under rib. No answers…. My life has been horrible since.”
Jill:
“…my energy levels have dropped too.”
Jen:
“I had TAH kept my ovaries (boy, that was a battle)…. I have had so many problems since…. I truly feel awful. My energy levels are just depleted. I’m dealing with idiot doctors rift now plus I am too tired to go to all these specialists…. I also have severe rib pain right and left. I have bowel problems too and the nausea and fatigue is hell.”
Irene:
“Ever since HYSTERECTOMY my whole personality has changed, gone from an outgoing lady to a hermit rarely interested in socialising and I have little energy and gone from 60kg to 70kg.”
Annele:
“Had my surgery in 2010, compared to photos of me and my energy levels, sex live, I have aged about 10 years in a 5 year period. My mother also went for her hysterectomy during 2012, she experienced similar side effects.”
Sharon:
“I can hardly get out of bed. I have no appetite, no energy, and I feel awful.”
Elaine:
“I ache constantly, I still get intense flashes and my energy level has gone from active (pre-surgery) to minimal…..I am so sleep deprived and so sore….I feel I was not thoroughly informed and this surgery was the biggest mistake! I cry and yearn for who I was a year ago.”
Julie:
“Ever since surgery I had so much pain, discomfort, fatigue, and now depression. I used to be real busy with my family going outdoors for hunts, fishing and picnics. Now days I just barely do anything and my whole life has changed. My health has just been going down.”
Lyn:
“After 3 months post surgery, I had to retire my full time profession as a licensed therapeutic massage therapist due to fatigue, lower back, sacroiliac joint, hip, leg and foot pain!… My balance has been compromised and have had (4) falls since surgery…. I use to enjoy my walks with my dog and make attempts daily, but I become winded and fatigued almost instantly….”
Sue:
“My health just continues to decline. I was the most active person before this surgery, now I do nothing most days. I’m very concerned about my bowel issue and the relentless fatigue.”
Angela:
“I saw my mother destroyed by a hysterectomy at 38. This has been going on for decades and the denial has to stop. Women don’t even have to tell me they’ve had one. I can see it – in their faces, their hair, their figures, their lack of vitality.”
Jacqualine:
“take ambien to sleep”
Marlo:
“I can’t sleep at night.”
KA:
“taking a sleep aide”
Rebecca:
“Can’t sleep, wake up with headaches every day. Having major sweats, Loosing my hair and my mind!”
I caution any woman who is told she needs a hysterectomy and/or oophorectomy or is considering one to heed these comments. With the gross overuse of these surgeries, chances are she’s being sold a false bill of goods. It’s not always a good idea to rely solely on your doctor’s advice as Someone
Who Cares cautions:
“After 40 years of enduring this “disabled” existence, it breaks my heart that no matter how many of us try to warn other women, in various ways, the number of these destructive surgeries continues to increase, not decrease.”
A complete list of my articles can be found here. The HERS Foundation is a good resource for understanding the lifelong functions of the female organs. It also has information about gynecologic conditions and treatment options. These two sites, Gyn Reform (especially the studies/citations link) and Ovaries for Life, are excellent resources about the gross overuse and harm of ovary removal or hysterectomy induced loss of ovarian function.
Share your Story
If you have a hysterectomy story, please consider sharing it on Hormones Matter.
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, like it, please help support it. Contribute now.
Yes, I would like to support Hormones Matter.
This article was first published in April 2017.



You might be interested in












 DES is not something of the past. People who have been exposed to this drug years ago are battling with health issues and fighting for their lives as I’m writing this blog post. Who knows what health problems the grandchildren of the mothers who were prescribed this drug will have to deal with as they grow up. I want my daughters to receive adequate medical care and monitoring if they ever have to suffer the consequences of this drug. This is why together with my husband we support the great work done by the very few International DES Action Groups who are providing valuable information and are advocating for the DES victims.
DES is not something of the past. People who have been exposed to this drug years ago are battling with health issues and fighting for their lives as I’m writing this blog post. Who knows what health problems the grandchildren of the mothers who were prescribed this drug will have to deal with as they grow up. I want my daughters to receive adequate medical care and monitoring if they ever have to suffer the consequences of this drug. This is why together with my husband we support the great work done by the very few International DES Action Groups who are providing valuable information and are advocating for the DES victims.






