COVID-19 Encephalitis
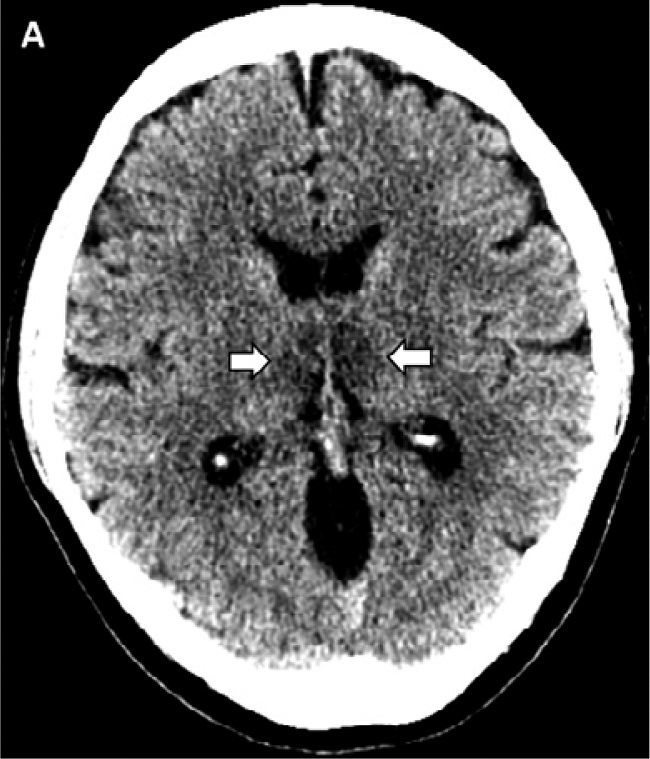
A recent article, posted online, described a woman in her 50s who had traditional symptoms of COVID-19 at first but then developed an altered mental state. She was studied by MRI that reportedly showed capillary hemorrhage (no stroke) involving a part of the brain known as the thalamus. Another article reported the radiological study of 56 patients with the thiamine deficiency brain disease known as Wernicke encephalopathy (WE). MR imaging findings reported that “80 % of the patients had evidence of symmetrical lesions in the medial thalami”, part of the brain which might justifiably be referred to as the part that computes a defensive, adaptive response.
Experimental thiamine deficiency in animals is a classical model for the study of metabolic encephalopathy and selective cell loss of the brain resulting from a generalized low-grade oxidative deficit. Late stages are characterized by hemorrhage in the brain and on day 13 of the experiment, tissue damage and hemorrhage was found in the thalamus. In a study of experimentally induced thiamine deficiency in mice, petechial hemorrhage was found in the brain tissues. Of course, it is not possible to tie these references together to indicate that the encephalopathy resulting from COVID-19 is due to thiamine deficiency. However, taken as a whole, they support the idea that the mental symptoms might well be a reflection of a brain energy deficit arising from a failed initiation of an automatic, defective defense program.
The question then arises: is there evidence for thiamine deficiency in other virus diseases? Wernicke encephalopathy has been described in AIDS patients, a disease that has been associated with viral cause. However, the lifestyle and diet of such patients is often questionable and may confuse the issue. Chronic hepatitis B, a viral disease, is an international health concern that results in liver failure and death. Indirect evidence suggested a relationship between thiamine treatment and aminotransferase levels (a laboratory test that indicates faulty energy metabolism), a report begging for clinical trial with megadose thiamine. Patients with sepsis are frequently thiamine deficient. This deficiency can cause congestive heart failure, peripheral neuropathy, Wernicke encephalopathy and gastrointestinal beriberi concomitantly, because it results in energy deficit. This should alert emergency room physicians to such a possibility with COVID-19, particularly with the more severe symptoms.
The point that I am trying to make here is that our conventional approach to disease may be catastrophically wrong. The symptoms, particularly those that are obviously related to brain function, arising from COVID 19 may be just expressions of a defensive war where failure spells death and recovery spells victory. The potential involvement with thiamine metabolism strongly suggests energy deficit as the underlying mechanism and that treatment should be aimed at “supporting the defense” by providing its stimulation instead of trying to find a means of killing the virus.
Drug Related Thiamine Deficiency
Drug-nutrient interactions have the potential to cause serious adverse events but unfortunately they receive little attention during drug development. Their importance was highlighted when the clinical trial of a drug had to be terminated because it was found that it interfered with thiamine absorption. The authors screened 1360 compounds, including many clinically used drugs and identified 146 that had this inhibitory reaction. The antibiotic metronidazole (Flagyl) is converted to a thiamine analog (a nearly identical formula), with consequent vitamin B1 antagonism, thus explaining how “toxicity” is produced by this drug. Serum thiamine levels were significantly lower in a group of patients with neurological symptoms receiving chemotherapy for gastrointestinal cancer. Perhaps the use of pharmacotherapy is another example of a fundamentally inappropriate treatment of symptoms without addressing the real issue.
We are beginning to understand that the organizational capacity of the brain in setting up a defense against a lethal microorganism requires an enormous amount of energy. Perhaps it is the present preoccupation with finding a name for a disease, based on its locality in the body that diverts our attention. A good example was published some years ago in Japan. Since the early 1960s a peculiar neurological disease became prevalent throughout Japan. It went by the name of subacute myelo-optico-neuropathy (SMON), later to be found due to the prescription of a drug called clioquinol for diarrhea. Apparently the cause of the disease had been ascribed to a virus as early as 1978. It should be apparent that discussing differences in the cause of disease would not matter nearly as much if a nutraceutical approach to treatment were to be adopted. The concept is reinforced by the information on television that 70% of COVID deaths occur in the black community where poverty and malnurition tend to go hand in hand. It would explain the reason why some people have only mild symptoms while others succumb, why concomitant disease and aging are risk factors. Could it be that all disease is just a temporary lack of ATP (sometimes referred to as the energy currency) arising from nutritional error, coupled with genetic risk: that nutraceuticals are the ubiquitous treatment for all?
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, like it, please help support it. Contribute now.
Yes, I would like to support Hormones Matter.
Image credit: COVID-19–associated Acute Hemorrhagic Necrotizing Encephalopathy: CT and MRI Features


You might be interested in