More About Eosinophilic Esophagitis
Seeing some of the comments following the appearance of my post Eosinophilic Esophagitis May Be a Sugar Sensitive Disease, it seemed that it was necessary to provide a little more explanation for how the conclusions were reached. Hopefully this may produce less misunderstanding.
Compartmentalized Medicine
The present model for disease is being rapidly outdated, so let me first of all review how a diagnosis is made in modern medicine. When a patient pays a visit to a physician, a medical history is recorded. The history begins by the patient describing symptoms, the sensory afflictions experienced since the loss of health began. This is followed by a physical examination when the physician is looking for evidence of malfunction. For example, this may include finding enlargement of a given organ, point tenderness when pain is elicited or a neurological deficit. Family history and the history of previous illnesses are both taken into account. The physician may or may not have a working idea of the nature of the disease process at this stage and a series of laboratory tests are requested. All of this is put together and the physician then has to consider what is generally referred to as a differential diagnosis. Which part of the physical examination, combined with the tests, all point conclusively to a diagnostic category?
This method of making a diagnosis was derived from the Flexner report initiated by Rockefeller in 1910. It was adopted from the German method in which laboratory confirmation was emphasized. This gave rise to the methodology that we now call “scientific medicine”. The symptoms, signs and laboratory reports are then put together and a given disease is named as the most likely fit.
So let us examine for a moment how this confuses us. All sensations are perceived in the brain and symptoms are merely a method by which the brain/body provides a warning that something is wrong. The “wrongness” has to be interpreted. In the present model, each constellation of symptoms, signs and laboratory reports are then given a name. For example, because somebody by the name of Parkinson was the first to describe a given constellation, it is called Parkinson’s disease, even though the underlying cause is completely unknown. Research has been aimed at finding a cure for that disease without giving full recognition to the fact that the constellation of findings overlaps with the constellations exhibited in other brain diseases, each being named separately. Furthermore, if the constellation points to an organ as the seat of a given problem (such as the intestine), the patient is referred to a specialist (a gastroenterologist) whose practice is confined to diseases of that organ (organic disease). An attempt to improve the symptoms by prescribing drugs is the chosen method, without considering the complex connection of the sick organ with the brain. An “anti-inflammatory” drug is prescribed, without asking why or what caused the organ to become sick.
In the case that I wrote about previously, the disease process called eosinophilic esophagitis or EoE, results from ingesting food. The presently accepted cause is “food allergy”.
Understanding Disease Differently: A Connected System
Let me provide an example to illustrate the change in perspective that occurs if the whole person is considered. On one of these posts a mother reported that her daughter had eosinophilic esophagitis, “associated with idiopathic gastroparesis” (partial or complete paralysis of the intestine). The word idiopathic stands for the simple sentence “the cause is unknown”. Evidently, no attempt had been made to connect the two conditions together. Is it likely that two unusual conditions will exist at the same time in one individual? By recognizing that the brain is always involved with body disease and brain disease is always involved with the body, it is possible to provide a solution for a connection between eosinophilic esophagitis and gastroparesis. It depends completely on an understanding of the profound genius of the brain/body interconnection.
The post that led to all of these comments asks the question, is this disease caused by the ingestion of sugar? We know that ingestion of sugar can easily induce thiamine deficiency because we have the ancient model of beriberi where white rice (without its surrounding cusp) ingestion, consumed as a staple, was found to be the cause. (Rice grain is starch and is broken down in the body to glucose. The cusp around the grain contains the vitamins. When the cusp of the rice is removed, as it is in white rice, the vitamins are removed leaving only the starch, which is converted to glucose.)
Digestion: Where Mechanical Meets Chemical
The vagus nerve is the 10th cranial nerve. Its action, initiated in the lower part of the brain, is to send outgoing messages to the spleen, an important organ that is used for controlling inflammation. The vagus nerve uses a neurotransmitter called acetylcholine and it also deploys messages to the esophagus and the entire intestinal tract. The wave pattern in the respective parts of the intestine that is induced by this nerve is called peristalsis. It pushes the contents along while the complex process of digestion occurs. Without going into details, the synthesis of acetylcholine depends on vitamin B complex, dominated by thiamine. Without thiamine, there is less acetylcholine and without this vital neurotransmitter, the control of inflammation and peristalsis in the esophagus, the intestinal tract, or both, are all compromised.
Eosinophilic Esophagitis and Food Allergy
In EoE, food sensitivity, occurring for whatever reason and known as food allergy, is causing inflammation that might occur in either the esophagus or any other part of the intestinal tract. When it occurs in the intestine it is called eosinophilic enteritis. Although the mechanism is the same, the locality differs but the esophagus is more commonly the affected part. The inflammatory response gets out of control because the vagus nerve, lacking acetylcholine to transmit the necessary information, is failing to suppress esophageal inflammation by sending a proper message to the spleen. The association of eosinophilic penetration into the intestinal tissue is part of the inflammation and it is interesting that a similar event has been associated with asthma in bronchial tubes. Asthma was a recurrent problem in the history of my patient.
Like the famous poem:
“for the want of a nail a shoe was lost; for the want of a shoe a horse was lost; for the want of a horse a battle was lost; for the want of a battle a kingdom was lost”.
To paraphrase this in biochemical terms “for the want of thiamine (vitamin B1), action of the citric acid cycle (engine of the cell) was lost; for the want of the citric acid cycle, acetylcholine (neurotransmitter) was lost; for the want of acetylcholine, suppression of inflammation was lost; for the want of acetylcholine, normal peristalsis (wavelike action) in the esophagus and intestinal tract was lost.
The loss of the peristaltic wave in the intestine was given the name “idiopathic gastroparesis”, a clear indication by the diagnostician that “its cause is unknown”. Like the blind men and the elephant the present medical model looks at a segment of the problem and fails to see the big picture. The trouble with this failure to understand the full nature of the problem is because we have divided brain disease from body disease. If it is suspected that the brain is the cause of the problem and all laboratory studies are negative, it is assumed that the symptoms are psychosomatic in nature and have been “imagined by the patient”. When the patient is told that it is “psychological”, it naturally induces anger.
My patient’s symptoms, recurring through infancy to the age of 8 years, were thought to be psychosomatic until endoscopy revealed the esophagitis. The “psychosomatic symptoms” were resulting from thiamine deficiency affecting the brain. His dramatic growth spurt during treatment strongly suggested that the autonomic (automatic) nervous system was at the seat of the complex problem. That conclusion can be supported by the medical literature concerning a well known genetically determined disease called Familial Dysautonomia, a disease whose clinical course results in growth failure. In the case of my patient, the dysautonomia was reversible and the result of thiamine deficiency, hence the growth spurt.
Nobody is looking for evidence of a vitamin deficiency because it has been assumed that that kind of disease is of only historical interest. This idea is so impregnated in the modern medical psyche that we can actually miss such a diagnosis when it is staring us in the face! That was the case here and may be the case in many other instances of eosinophilic esophagitis or enteritis.
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, like it, please help support it. Contribute now.
Yes, I would like to support Hormones Matter.
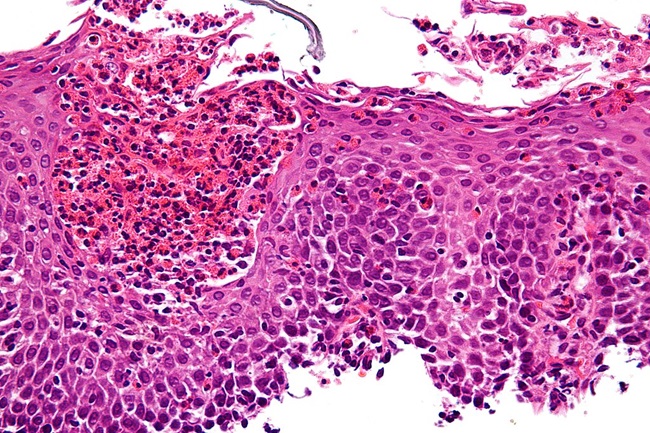
Very high magnification micrograph of eosinophilic esophagitis.
Nephron, CC BY-SA 3.0, via Wikimedia Commons.




{kind=link}
You might be interested in


