
There is an old saying “for any workman who has only a hammer for a tool, everything is a nail”. Thus, I am in danger of writing article after article about one vitamin, B1, or thiamin/thiamine, but write I must. Thiamine is critical for energy production and the energetic demands of pregnancy are substantial. Insufficient thiamine during pregnancy can and does have negative impacts on both maternal and fetal health. Both Dr. Marrs and I have written about this previously, but it bears exploring further. Before we begin, however, let us review a few concepts.
Energy to Respond
In order to understand its therapeutic use in the treatment of many different conditions, you have to understand its function and how it differs from “taking medicine”. Let me first remind you that we live in a hostile environment to which we have to adapt in order to survive. Infection, trauma, weather, work assignments and a variety of changes in life’s journey (stress) have to be met as they occur. Assuming that our genetically determined “blueprint” is intact, all we require is energy. To meet the pressure of stress, an automatically increased supply of energy is necessary. Food provides us with fuel that must be burned (oxidized) in supplying that energy and thiamine is essential in igniting the fuel.
When we are attacked by a microorganism, the brain organizes a comprehensive defensive mechanism that we refer to as an illness or a disease. With trauma, healing requires increased energy so that the healing process can proceed. Let it be clearly understood once again that our food provides both the fuel and the vitamins that enable oxidation to supply the required energy. I have come to the conclusion that illness is either a genetically determined error in the DNA code, a failure to synthesize the energy requirement to meet stress, or a combination of the three. If we are attacked by a microorganism, a healthy organism defeats the foe. This is by no means a new idea. It just has not been put into practice, so we are still stuck with the antiquated concept that each disease is represented by a collection of symptoms and physical signs with a unique cause in each case that must be researched to find the magic cure. In order to understand why a thiamine supplement is so protective in pregnancy, I must try to show that any form of stress requires a genetically determined resistance and energy. It is illustrated by a case in my own clinical experience.
When Genetics, Trauma and Diet Collide: Cataracts and Galactosemia
Some years ago, a 6-year old boy was referred to me by an ophthalmologist, because he had been found to have cataracts in both eyes. The ophthalmologist knew that this could be a manifestation of a rare genetically determined disease known as galactosemia and had asked me to research it. There is a sugar in milk called lactose. When milk is consumed, the lactose is converted to galactose that is then broken down by a recessive gene inherited from each of the parents. In order to bear a child that has the potential to have the disease, the child must have obtained a gene from each parent. With two genes, the galactose accumulates in the blood and affects the eye, causing the density known as cataract.
The level of galactose can be determined in the laboratory and in the case of this child, it was in the normal range, at the time of the study. In the meantime, however, the laboratory had been asked to check the presence of the abnormal gene. It was reported that he had only one copy of the gene. With only one copy, the child was classified as a carrier and on general principles, he could not have the disease. So I sat down with the child’s mother to ask her about the diet that she had been giving and I found that she had a tremendous faith in the health manifestations of milk. Therefore she had insisted on multiple glasses of milk for the child. In addition the child had experienced a head injury with a fractured skull. When he returned to school, the school nurse had insisted that he have eye testing every two weeks because, she said “people go blind after an injury like this”. Whether this was an accurate statement or not, the child’s vision was perfectly normal immediately after his discharge from hospital. Three months later there was a dramatic change, causing her to refer the child to the ophthalmologist who had discovered the cataracts. I had to conclude that the combination of trauma, genetic risk and unknown dietary indiscretion combined to cause the disease. The “stress” of the head injury, or the genetic carrier state, or the excessive intake of milk, would not be damaging on their own. It was their coincidental relationship that precipitated the cataracts.
The Energetic Demands of Pregnancy
In 2013, I received a letter from Dr. John Irwin an OB/GYN specialist in Connecticut and his remarkable book: The Natural Way to a Trouble-Free Pregnancy: The Toxemia-Thiamine Connection. The letter said:
Dear Dr. Lonsdale,
I am writing to you, because I have found another mortal being who is particularly interested in the biological activities of thiamine. I had previously thought that I was nearly the loan believer in the benevolent effects of thiamine, particularly for the treatment and prophylaxis of the toxemias of pregnancy and its many associated problems. I had even written to the chief of the Cleveland Clinic OB-GYN about the “miracles” I was performing and offered to work with him in further development of the concepts, but my information seems to have experienced obstacles.
After Dr. Irwin had retired, he spent 25 years in the Commonwealth of the Northern Mariana Islands where he had been concentrating on the use of what he called “megathiamin, 100 mg daily” in the prevention of toxemia and many other complications of pregnancy. His first patient was introduced to him by an introductory meeting with a group of island doctors who were all American board-certified in their specialties. The patient had severe preeclampsia, had been sick for six weeks and was essentially moribund at 36 weeks of gestation. She also had severe heart disease and he recognized the compound symptoms of thiamine deficiency disease. In the face of the open skepticism of the other physicians, he started her on a 100 mg pill of thiamine daily. He reported that she was cured in six days. She had some fetal distress on the seventh day and was delivered of a 3 lbs. 12 oz. baby by cesarean section. The infant’s Apgar was 10-10, an extraordinary result in a situation where death of both mother and infant would be the expected outcome.
He then started all his patients on “prophylactic megathiamin” at the third trimester and he reported that it prevented the development of every type of toxemia completely, including eclampsia, preeclampsia, intrauterine growth retardation of the fetus, premature delivery, fetal death, premature rupture of membranes and in fact virtually any pregnancy complication. To anyone that contemplates pregnancy and can overcome her expected skepticism, this book is an absolute essential.
Thiamine, Energy, and Pregnancy
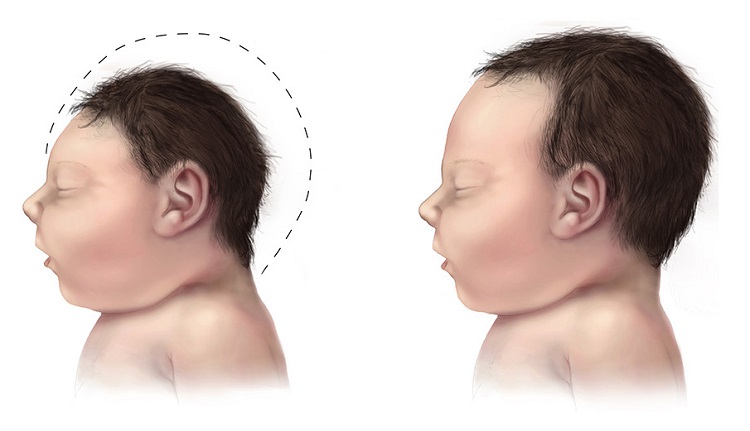
I believe that we can offer a rational explanation of what superficially appears to be “miraculous”. In many posts on this website I have commented on the energy relationship between stress and maintenance of well-being. There must always be a complete balance between energy synthesis and its utilization. In good health, the rate of synthesis automatically accelerates to meet any increased demand, although there must be a normal limit to that capacity. The stress in pregnancy is enormous. The mother is feeding her fast-growing baby as well as herself, giving rise to a marked increase in energy demand. Thiamine is the key to energy synthesis from the oxidation (burning) of glucose. Her physiology must meet this ever increasing demand to full-term. The failure of this equation obviously imperils both mother and fetus and it also explains many of the complications observed in the neonate’s immediate and future development. The dysregulation of body organs by the energy deficient brain explains the multiplicity of the complications because all of them have a common cause.
Unfortunately, many people have concluded that taking sugar will increase energy production by “throwing fuel on the fire”, a fact that has led to a great deal of energy deficiency illness. There has to be a normal glucose/thiamine ratio for healthy oxidation. Just as an excess of gasoline introduced into the cylinders of a car produces inefficient engine performance, an excess of glucose induces illness. If we insist on ingesting empty calories, we must optimize the glucose/thiamine ratio by supplementing thiamine, thus explaining Dr. Irwin’s success in eliminating many of the common complications associated with pregnancy.
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, like it, please help support it. Contribute now.
Yes, I would like to support Hormones Matter.
This article was published originally on February 11, 2019.




You might be interested in

















.jpg){kind=link}