I have read a criticism that thiamine deficiency is “too simple” to explain the devastating nature of the post Gardasil illnesses or the systemic adverse reactions to some medications. Sometimes, it is the simple and overlooked elements that are the most problematic.
Understanding Thiamine’s Role in Complex Adverse Reactions – The Limbic System
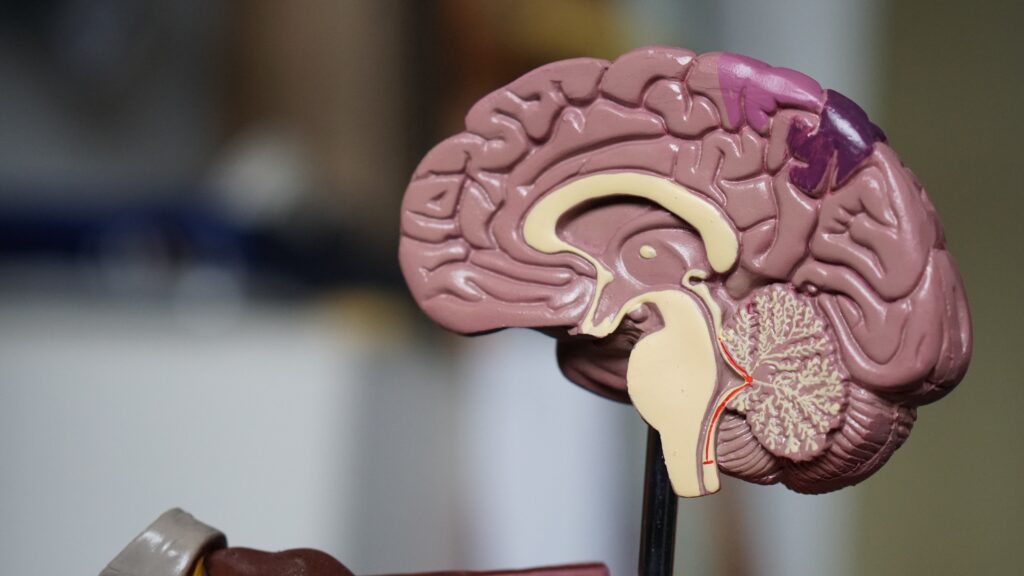
The lower part of the brain, called the brainstem, is a like computer, controlling the most basic aspects of survival, from breathing and heart rate, hunger and satiety, to fight or flight and reproduction. This computer-like function within the brainstem is called the autonomic system (ANS). The ANS together with the limbic system act in concert to regulate our most basic survival functions and behaviors. Both require thiamine to function.
Postural Orthostatic Tachycardia Syndrome or POTS , a type of dysautonomia (dysregulation of the autonomic system) seems to be the among the commonest manifestations of the Gardasil effect. Many cases have been diagnosed already, while others present all of the symptoms but have yet to receive a diagnosis. Dysautonomia and POTS have also been observed with adverse reactions to other medications, as well. Dysautonomia and POTS, at the most basic level, represent a chaotic state of the limbic-autonomic system. Let me explain.
Fragmented Fight or Flight
The brainstem autonomic system together with the limbic system enable us to adapt to our environment, presiding over a number of reflexes that allow us to survive. For example, fight-or-flight is a survival reflex, triggered by perception of a dangerous incident that helps us to kill the enemy or escape. This kind of “stress event” in our ancestors was different from that we experience today. Wild animal predators have been replaced by taxes/business deadlines/rush hour traffic etc. These are the sources of modern stress. The beneficial effect is that the entire brain/body is geared to physical and mental response. However, it is designed for short term action and consumes energy rapidly. Prolonged action is literally exhausting and results in the sensation of fatigue. In the world of today where dietary mayhem is widespread, this is commonly represented as Panic Attacks, usually treated as psychological. They are really fragmented fight-or-flight reflexes that are triggered too easily because of abnormal brain chemistry.
Thiamine and Oxidative Metabolism: The Missing Spark Plug
Our brain computers rely completely on oxidative metabolism represented simply thus:
Fuel + Oxygen + Catalyst = Energy
Each of our one hundred trillion body/brain cells is kept alive and functioning because of this reaction. It all takes place in micro “fireplaces” known as mitochondria. Oxygen combines with fuel (food) to cause burning or the combustion – think fuel combustion engine. We need fuel, or gasoline, to burn and spark plugs to ignite in order for the engines to run.
In our body/brain cells it is called oxidation. The catalysts are the naturally occurring chemicals we call vitamins (vital to life). Like a spark plug, they “ignite” the food (fuel). Absence of ANY of the three components spells death.
Antioxidants like vitamin C protect us from the predictable “sparks” (as a normal effect of combustion) known as “oxidative stress”. Vitamin B1, is the spark plug, the catalyst for these reactions. As vitamin B1, thiamine, or any other vitamin deficiency continues, more and more damage occurs in the limbic system because that is where oxygen consumption has the heaviest demand in the entire body. This part of the brain is extremely sensitive to thiamine deficiency.
Why Might Gardasil Lead to Thiamine Deficiency?
We do not know for sure how Gardasil or other vaccines or medications have elicited thiamine deficiency, but they have. We have two girls and one boy, tested and confirmed so far. More testing is underway. Thiamine deficiency in these cases may not be pure dietary deficiency. It is more likely to be damage to the utilization of thiamine from as yet an unknown mechanism, affecting the balance of the autonomic (automatic) nervous system. It is certainly able to explain POTS (one of the many conditions that produce abnormal ANS function) in two Gardasil affected girls. Beriberi, the classic B1 deficiency disease, is the prototype for ANS disease. Administration of thiamine will not necessarily bring about a cure, depending on time since onset of symptoms, but it may help.
Thiamine Deficiency Appetite and Eating Disorders
Using beriberi as a model, let us take appetite as an example of one of its many symptoms. When we put food into the stomach, it automatically sends a signal to a “satiety center” in the computer. As we fill the stomach, the signals crescendo and the satiety center ultimately tells us that we have eaten enough. Thiamine deficiency affects the satiety center, wrecking its normal action. Paradoxically it can cause anorexia (loss of appetite) or the very opposite, a voracious appetite that is never satisfied and may even go on to vomiting. It can also shift from anorexia to being voracious at different times within a given patient. That is why Anorexia Nervosa and Bulimia represent one disease, not two.
Thiamine Deficiency, Heart Rate and Breathing
The autonomic nervous system, responsible for fight or flight, regulates heart activity, accelerating or decelerating according to need. So heart palpitations are common in thiamine deficiency. Its most vital action is in control of automatic breathing and thiamine deficiency has long been known to cause infancy sudden death from failure of this center in brainstem.
Thiamine Deficiency and Sympathetic – Parasympathetic Regulation
The hypothalamus is in the center of the brain computer and it presides over the ANS, as well as the endocrine (hormone) system. The ANS has two channels of communication known as sympathetic (governs action) and parasympathetic (governs the body mechanisms that can be performed when we are in a safe environment: e.g. bowel activity, sleep, etc.). When the ANS system is damaged, sometimes by genetic influence, but more commonly by poor diet (fuel), our adaptive ability is impaired. A marginal energy situation might become full blown by a stress factor. In this light, we can view vaccines and medications as stress factors. From false signal interpretation, we may feel cold in a warm environment, exhibiting “goose bumps on the skin”, or we may feel hot in a cold environment and experience profuse sweating. The overriding fatigue is an exhibition of cellular energy failure in brain perception.
Sometimes, it really is the simple, overlooked, elements that cause the most devastating consequences to human health. Thiamine deficiency is one of those elements.
To learn more about thiamine testing: Thiamine Deficiency Testing: Understanding the Labs.
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, like it, please help support it. Contribute now.
Yes, I would like to support Hormones Matter.
Photo by Robina Weermeijer on Unsplash.
This article was published originally in October 2013.




You might be interested in











{kind=link}