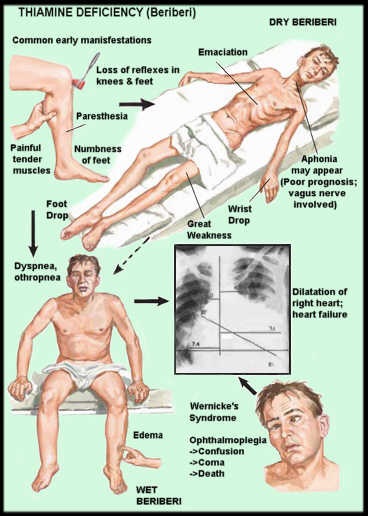
A Case of Classic Beriberi in America

A desperate mother sent me an email about her 23-year-old son and it was easy to recognize that this young man had full-blown beriberi. You may or may not know that beriberi is well known as a vitamin B1 deficiency disease. Because the medical profession is convinced that this disease never occurs in America, it is usually not recognized for what it is. He had seen many physicians without success. I want to record the majority of his symptoms to show that they are surprisingly common and are usually ascribed to a “more modern” diagnosis. I have christened beriberi as the “great imitator” and I am sure that the reader will readily recognize the common nature of these symptoms, presented below in the form of a Table. It is important also to understand that these symptoms can occur for other reasons, but thiamine deficiency is widespread.
| collapsing fatigue | confusion |
| panic attacks | loss of balance |
| blurred vision | cluster headaches |
| hair loss | jaundice at birth |
| infantile colic | migraines |
| poor intestinal motility | bloating |
| severe calf pain | joint pains |
| weakness | salt craving |
| cold extremities | chemical sensitivity |
| POTS | severe pain sensitivity |
I want now to describe some of the features reported by this mother that were extremely important major clues. She described her son, when in good health, as 6’2”, 175 pounds, extremely athletic with “amazing hand-eye coordination and finishing college with high honors”.
As a result of his undiagnosed illness, his weight had dropped to 133 pounds. Because thiamine governs energy metabolism, an intelligent brain consumes a great deal. Of course, compromised energy production can occur for reasons other than thiamine deficiency. But there were very strong clues for beriberi. The mother described how her son
“…went out drinking with friends. The next day he could barely sit up in the car or stand. We were all commenting on why he was having such an extreme hangover”.
Alcohol would certainly exaggerate an existing thiamine deficiency. It is a well-known association. The symptoms were intermittent, rising and falling “for no apparent reason”. For example, she said that he was
“able to play sports, then lose his balance, become weak and complain of blurred vision”.
The reason for this is because the physical activity was demanding energy that could not be supplied because of the thiamine deficiency. He had jaundice at birth, now known to be because of inefficient oxygen utilization. This would indicate poor maternal diet in pregnancy or a genetic mechanism involving thiamine absorption. So-called panic attacks are common in the modern world and are absolute indicators of poor oxygen utilization in the brain. Under these conditions the reflex known as fight-or-flight would be initiated and this is what is being called panic attacks. The blurred vision would go along with this too.
Beriberi Is a Form of Dysautonomia
We have two nervous systems. One maintains what we call willpower and is known as the voluntary system. The other one is known as autonomic and is entirely automatic and outside willpower. This system controls all the organs within the body. It explains why there are so many symptoms involving many parts of the body. This is because of the loss of signaling power between the organs and the brain. A lot of energy is required to run this system and explains why the autonomic nervous system is affected in beriberi. POTS is one variety of dysautonomia. This young man craved salt and that too is a form of dysautonomia is known as cerebral salt wasting syndrome, explaining the natural craving.
Is There a Help From the Laboratory?
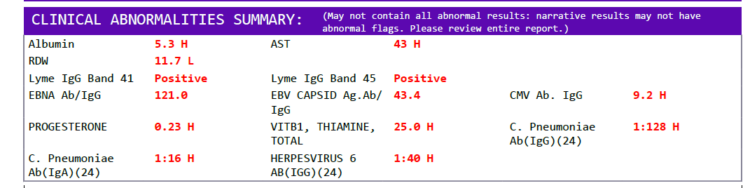
The answer to this is no, as long as physicians refuse to recognize that beriberi is common in America. This unfortunate young man was diagnosed almost certainly as psychosomatic. The disease has a very long morbidity with symptoms shifting up and down according to the state of energy metabolism on a day-to-day, week-to-week and month-to-month basis. The laboratory has to look for it because the standard tests done only provide distant clues. It is the absence of the abnormal results that make it easy to conclude that this is “a psychologic disease”. For example, it was reported that this young man had an elevated vitamin B12 and a mildly elevated CRP. I cannot give the complex details here, but both are peculiarly related to energy metabolism and require understanding in order to fit them into the pattern of diagnostic clues. I have reported these facts elsewhere.
What Is the Hope of Normal Health in This Person?
It stands to reason that the first thing is proper diagnosis and a knowledge of the widespread symptomatology, including their fluctuation. As long as he continues to take alcohol and sugar, he will never get his health back even if he supplements with thiamine. He is in danger of developing the classical brain disease known as Wernicke’s Encephalopathy. This state of the disease almost certainly involves cellular damage that cannot be repaired. It is therefore very urgent to understand the self-responsibility that is required. He has to learn that alcohol is potentially lethal for him. There is undoubtedly a genetic relationship between alcoholism and sugar craving and it is probably true that a search for the genetic relationship would at least be helpful in understanding the nature of this disease.
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, like it, please help support it. Contribute now.
Yes, I would like to support Hormones Matter.
Image by NoName_13 from Pixabay.
This article was published originally on August 9, 2017.




You might be interested in



























{kind=link}