Cipro, Levaquin and Avelox are Chemo Drugs

When I first heard people referring to fluoroquinolone antibiotics (Cipro, Levaquin, Avelox, Floxin and a few others) as “chemotherapy drugs,” I thought that they were exaggerating or incorrect. After all, fluoroquinolones are used to treat urinary tract infections, traveler’s diarrhea, anthrax, and other bacterial infections, not cancer. But then I started to do some research into how fluoroquinolones work and I discovered that they cause mitochondrial damage, which leads to oxidative stress and cell death (1, 2), they interfere with the DNA replication process of mitochondria (3), they disrupt tubulin assembly (4) and that they are being investigated for their tumor killing abilities (5, 6). I also found that all other drugs that have the same mechanism for action as fluoroquinolones – topoisomerase interrupters (FDA warning label, 7) (topoisomerases are necessary for proper DNA replication) – are used as chemotherapy drugs – topotecan, amsacrine, etoposide, etc. Fluoroquinolones are, truly, chemotherapy drugs – they just happen to be used as popular antibiotics. They can kill cancerous tumor cells because, in addition to killing bacterial cells, they also kill eukaryotic cells (8, 9).
Use of Fluoroquinolones for Cancer Treatment is Appropriate
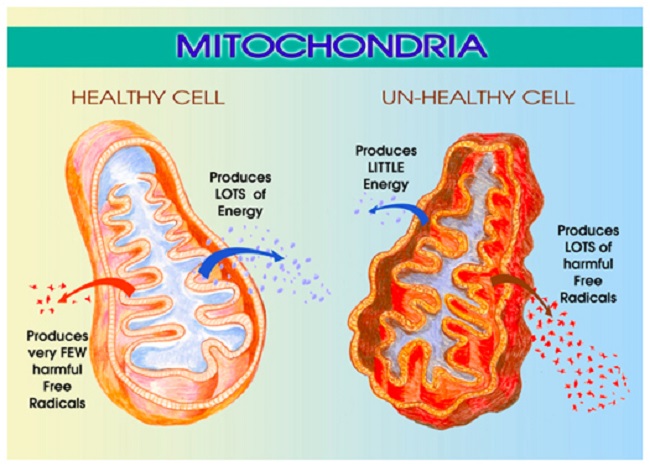
There are almost certainly some legitimate and reasonable uses for fluoroquinolones as chemotherapy drugs (10). As tumor killing agents, they may save lives of those with cancer. Unfortunately, they’re not as targeted as the chemotherapy drugs that are currently in use. Many chemotherapy drugs on the market specifically target quickly dividing cells – like tumor and hair cells; so they kill the cancer cells while leaving most other cells intact. Fluoroquinolones aren’t that precise. They indiscriminately kill cells throughout the body – including neurons and lymphocytes (11) (immune system cells). The mitochondrial DNA (mtDNA) replication process is disrupted by fluoroquinolones (3), and the disruption of that process leads to mitochondrial damage, oxidative stress and cell death (12). Fluoroquinolones are effective cell killers, but because they are indiscriminate cell killers, they are a step backward in chemotherapy drug technology.
Lousy Chemo Drugs? Let’s Use Them as Antibiotics for Everyone!
Because they are not particularly good chemotherapy drugs, fluoroquinolones are rarely used for the purpose of killing cancer cells. Instead, they are used as antibiotics. They are prescribed to treat sinus infections, bladder infections, strep throat, and they are even prescribed prophylactically (typically for future treatment of travelers’ diarrhea) when no infection is present. They kill bacteria, and are effective antibiotics, but they also damage mitochondria and destroy cells and therefore have many of the same side-effects as chemotherapy drugs, because, as noted above, they are chemotherapy drugs.
Side-Effects of Fluoroquinolones, and Other Chemotherapy Drugs
Some of the side-effects that fluoroquinolones share with chemotherapy drugs are (13, 14, 15, 16 and the FDA warning label for Ciprofloxacin – the warning labels for Levofloxacin and the other fluoroquinolones are similar):
- Exhaustion / Loss of energy / Fatigue
- Brain-fog / Loss of cognitive abilities
- Anemia
- Muscle Loss / Wasting
- Neuropathy / Peripheral Neuropathy / Fibromyalgia
Additionally, Fluoroquinolones destroy connective tissue, especially tendons. (17, 18, 19)
When one thinks of fluoroquinolones as chemotherapy drugs as opposed to antibiotics (yes, they do kill bacteria, but they should not be thought of in the same terms as benign drugs like penicillin and cephalosporins), many aspects of adverse reactions to fluoroquinolones make sense. Like several other chemotherapy drugs, there is a tolerance threshold (and/or lifetime limit) for fluoroquinolones (20, 21). Many people don’t react to their first dose of a fluoroquinolone. Rather, they tolerate the drugs up to a point – then they can no longer tolerate them and Fluoroquinolone Toxicity results. For fluoroquinolones, and possibly for other chemotherapy drugs, this tolerance threshold issue is because mitochondria are able to withstand a certain amount of damage before a disease state ensues. It is only after the tolerance threshold for damage is crossed that mitochondria stop adapting to harmful stimuli and a disease state ensues. (22)
Cellular Damage from Chemo Drugs can Lead to Cancer – Isn’t that Ironic?
Destruction of mitochondrial DNA can result in mitochondrial dysfunction and oxidative stress – which lead to apoptosis and necrosis of cells (23). When this occurs, a multi-symptom, chronic, autoimmune-disease-like reactions can occur (24, 25). However, if cell damage occurs but the cell does not die, but rather replicates the DNA errors, cancer can result (26, 27, 12).
Additionally, drugs that inhibit CYP450 liver enzymes [Cytochrome P450 enzymes metabolize xenobiotics and foreign chemicals from the body. (28)] leave people more susceptible to cancer-causing pathogens (29). Fluoroquinolones inhibit multiple CYP450 enzymes (30, FDA warning label). How ironic, isn’t it? Cancer can result from chemotherapy drugs. And when it is understood that fluoroquinolones are chemotherapy drugs that damage mtDNA and cause oxidative stress and apoptosis/necrosis, the irony of chemotherapeutic drugs causing cancer becomes horrifying, as opposed to thought-provoking.
Cellular Harm Results from Willful Ignorance About the Effects of Fluoroquinolones
There are articles that say that fluoroquinolones have an excellent safety record. (31) None of those articles look at the effects of these drugs on the mitochondria – the depletion of mtDNA, the oxidative stress that results from damaged mitochondria, the DNA damage that is caused by the oxidative stress, etc. In not looking at mitochondria, those articles are looking at the wrong things and they in no way negate the findings of the articles that note the deleterious effects of fluoroquinolones on human cells.
While it may be appropriate to give drugs that disrupt the process of mitochondrial DNA replication, have horrific side-effects and cause indiscriminate cell death, to people who are have cancer, it is absurd to give them to people who are healthy other than a minor infection. Even for major, difficult to treat infections, fluoroquinolones should be the drugs of last resort because of their effects on mitochondria. (1, 32) Chemotherapy drugs should be used exclusively in life-or-death situations. They should not be used frivolously or without true informed consent of the patient, or without awareness of the consequences of the drug on the part of both the physician and the patient. Protocols should be in place for ensuring that they are used appropriately and that all parties are aware of the consequences of the drugs.
Sadly, appropriate informed consent around fluoroquinolones involves a complete shift in how physicians and patients alike think about them. In order for the risks of taking fluoroquinolones to be properly acknowledged, all parties involved need to see, and acknowledge, that fluoroquinolones are chemotherapeutic drugs that cause mitochondrial destruction and cell death, and that they should not be used lightly. But because fluoroquinolones have been given out frivolously – 26.9 million prescriptions for oral and IV fluoroquinolones were given out in 2011 alone (33) for simple infections, I don’t foresee the shift in how they are perceived as an easy one. It must involve many doctors admitting that they have been prescribing these drugs incorrectly for decades, that they have been wrong about the severity of adverse effects, and that they have been misled about the risks of fluoroquinolones.
The Effects of Drugs on Mitochondria are Systematically Disregarded
It should also be noted that the effects of drugs on mitochondria are systematically disregarded. Mitochondrial function, and drug-induced dysfunction, is important to all areas of human health. An article published in Molecular Nutrition and Food Research entitled “Medication Induced Mitochondrial Damage and Disease” noted that the effects of drugs on mitochondria are ignored by both the drug companies and the FDA when reviewing drug safety. Because of this omission in review and oversight, human mitochondrial DNA have been repeatedly damaged by fluoroquinolones and other pharmaceuticals. The consequences of this are, as of yet, unknown. (Though it should be noted that mitochondria and the signals that they produce influence gene expression (35) and that an article published in Nature in July, 2013 entitled “Topoisomerases Facilitate Transcription of Long Genes Linked to Autism” showed that topoisomerase interrupting chemotherapy drugs effect the expression of genes linked to Autism.) We can only hope that the FDA’s failure to force drug reviewers to look at the effects of drugs on mitochondrial DNA isn’t horribly consequential.
Sources:
- Science Translational Medicine, “Bactericidal Antibiotics Induce Mitochondrial Dysfunction and Oxidative Damage in Mammalian Cells”
- British Journal of Cancer, “Ciprofloxacin Induces Apoptosis and Inhibits Proliferation of Human Colorectal Carcinoma Cells”
- Molecular Pharmacology, “Delayed Cytotoxicity and Cleavage of Mitochondrial DNA in Ciprofloxacin Treated Mammalian Cells”
- Current Medicinal Chemistry, “Recent Advances in the Discovery and Development of Quinolones and Analogs as Antitumor Agents”
- Inorganic Chemistry, “New uses for old drugs: attempts to convert quinolone antibacterials into potential anticancer agents containing ruthenium”
- Asian Pacific Journal of Cancer Prevention, “Comparative Evaluation of Antiproliferative Activity and Induction of Apoptosis by some Fluoroquinolones with a Human Non-small Cell Lung Cancer Cell Line in Culture”
- Mutation Research, “Ciprofloxacin: Mammalian DNA Topoisomerase Type II Poison In Vivo”
- The Journal of Biological Chemistry, “Cytotoxicity of Quinolones toward Eukaryotic Cells: Identification of Topoisomerase II as the Primary Cellular Target for the Quinolone CP-115,953 in Yeast”
- Antimicrobial Agents and Chemotherapy, “Effects of Novel Fluoroquinolones on the Catalytic Activities of Eukaryotic Topoisomerase II: Influence of the C-8 Fluorine Group”
- Urology, “Quinolone antibiotics: a potential adjunct to intravesical chemotherapy for bladder cancer”
- Nepal Medical College Journal, “Genotoxic and cytotoxic effects of antibacterial drug, ciprofloxacin, on human lymphocytes in vitro”
- Toxicology and Applied Pharmacology, “Mitochondrial abnormalities–a link to idiosyncratic drug hepatotoxicity?”
- National Cancer Institute, “Chemotherapy Side Effects Sheets”
- The Annals of Pharmacotherapy, “Peripheral Neuropathy Associated with Fluoroquinolones”
- Indian Journal of Psychiatry, “Levofloxacin Induced Acute Psychosis”
- Journal of Antimicrobial Chemotherapy, “Peripheral Sensory Disturbances Related to Treatment with Fluoroquinolones”
- The American Journal of Sports Medicine, “The Effect of Ciprofloxacin on Tendon, Paratenon, and Capsular Fibroblast Metabolism”
- Physical Medicine and Rehabilitation (PM & R) “Musculoskeletal Complications of Fluoroquinolones: Guidelines and Precautions for Usage in the Athletic Population”
- Laboratorie de Toxicologie, “In Vitro Discrimination of Fluoroquinolones Toxicity on Tendon Cells: Involvement of Oxidative Stress”
- Carcinogenesis, “Mechanisms of tolerance to DNA damaging therapeutic drugs”
- Non-Hodgekin’s Lymphoma Cyberfamily
- Molecular Interventions, “Mechanisms of Pathogenesis in Drug Hepatoxicity Putting the Stress on Mitochondria”
- Toxicology and Applied Pharmacology, “Mitochondrial abnormalities–a link to idiosyncratic drug hepatotoxicity?”
- Cleveland Clinic Journal of Medicine, “Mitochondrial cytopathy in adults: What we know so far”
- Antimicrobial Agents and Chemotherapy, “Ciprofloxacin Induces an Immunomodulatory Stress Response in Human T Lymphocytes”
- Scitable by Nature Education, “DNA Replication and Causes of Mutation”
- British Journal of Haematology, “Topoisomerase II Inhibitor Related Acute Myeloid Leukaemia”
- Mutation Research/Fundamental and Molecular Mechanisms of Mutagenesis, “Role of cytochromes P450 in chemical toxicity and oxidative stress: studies with CYP2E1”
- Europe Pubmed Central, “Role of cytochromes P450 in drug metabolism and hepatotoxicity.”
- Pharmacy Times, “Get to Know an Enzyme: CYP1A2”
- Expert Reviews, “Levofloxacin: update and perspectives on one of the original ‘respiratory quinolones’”
- Journal of Young Pharmacists, “Oxidative Stress Induced by Fluoroquinolones on Treatment for Complicated Urinary Tract Infections in Indian Patients”
- FDA Drug Safety Communications, “FDA Drug Safety Communication: FDA requires label changes to warn of risk for possibly permanent nerve damage from antibacterial fluoroquinolone drugs taken by mouth or by injection”
- Molecular Nutrition and Food Research, “Medication Induced Mitochondrial Damage and Disease”
- BBA, “Mitochondrial DNA Damage and its Consequences for Mitochondrial Gene Expression”
- Nature, “Topoisomerases Facilitate Transcription of Long Genes Linked to Autism”
Information about Fluoroquinolone Toxicity
Information about the author, and adverse reactions to fluoroquinolone antibiotics (Cipro/ciprofloxacin, Levaquin/levofloxacin, Avelox/moxifloxacin and Floxin/ofloxacin) can be found on Lisa Bloomquist’s site, www.floxiehope.com.
Participate in Research
Hormones MatterTM is conducting research on the side effects and adverse events associated with the fluoroquinolone antibiotics, Cipro, Levaquin, Avelox and others: The Fluoroquinolone Antibiotics Side Effects Study. The study is anonymous, takes 20-30 minutes to complete and is open to anyone who has used a fluoroquinolone antibiotic. Please complete the study and help us understand the scope of fluoroquinolone reactions.
Hormones MatterTM conducts other crowdsourced surveys on medication reactions. To take one of our other surveys, click here.
To sign up for our newsletter and receive weekly updates on the latest research news, click here.
What Else Can I Do To Help?
Hormones MatterTM is completely unfunded at this juncture and we rely entirely on crowdsourcing and volunteers to conduct the research and produce quality health education materials for the public. If you’d like help us improve healthcare with better data, get involved. Become an advocate, spread the word about our site, our research and our mission. Suggest a study. Share a study. Join our team. Write for us. Partner with us. Help us grow. For more information contact us at: info@hormonesmatter.com.
To support Hormones Matter and our research projects – Crowdfund Us – Buy an Unsubscription.


You might be interested in