An Open Letter Regarding Thiamine and COVID

Prior to the US election, in October of 2020, I found that the Biden campaign was interested in emailing me. I decided to try and get this letter setting out my concerns about COVID to Mr. Biden. I have no idea if he saw it or not. It is being published here as an open letter to whomever might consider implementing thiamine therapy in the prevention and treatment of COVID and other disease processes. It has been edited to fit the format of the website.
Dear Mr. Biden,
Greetings from Canberra Australia. I am writing to you because I believe I have something important to say about the pandemic, but find myself in somewhat of a dilemma. It may sound hard to believe but I think you may be the only person who can help.
I want to begin by telling you about Dr. Derrick Lonsdale. He is 96 years old, born in 1924. He began his medical career in England in 1948 and after emigrating to the U.S. spent 20 years practicing as a pediatrician at the Cleveland Clinic, which you visited recently. After leaving there he practiced privately, retiring at the age of 88 in 2013. He has written over 100 published papers. To this day he writes articles and helps people with their health problems through a website called Hormones Matter run by his colleague Dr. Chandler Marrs.
As a result of his experiences at Cleveland Clinic, Dr. Lonsdale became particularly interested in the subject of thiamine deficiency. As you may know, in the same way that vitamin C deficiency is linked to the disease scurvy and vitamin D deficiency is associated with rickets, thiamine, or vitamin B1, deficiency is responsible for the wasting disease beriberi. The common understanding is that this is a disease of the past and of a third world beset by malnutrition, which has been eliminated in the West by fortifying processed food such as flour with thiamine. As such it has seemingly passed out of the collective memory of modern medicine. Dr. Lonsdale on the other hand made the biochemical study of thiamine deficiency his life’s work.
Understanding Thiamine in the Context of Mitochondria
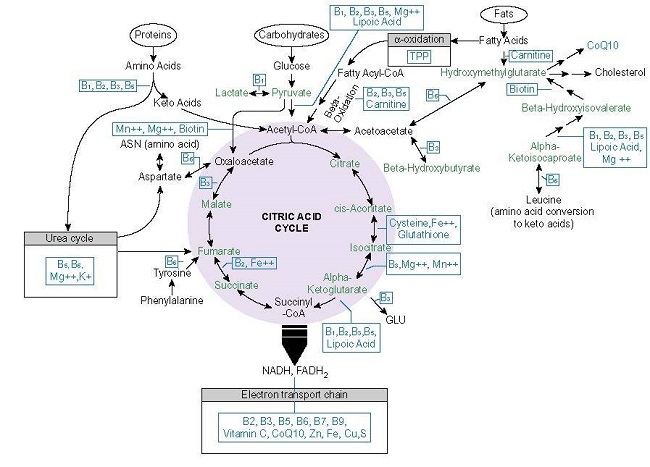
Each of the trillions of cells that make up the body contain mitochondria – self-contained electrochemical machines which take in fuel and oxygen supplied by the blood and use them to generate an electric charge – effectively a battery. This charge is used to supply energy in a chemical form usable by the cell to allow it to function. The other end-products are water and carbon dioxide – this is respiration at the cellular level. The process involves a series of chemical reactions, each reaction requiring the presence of an enzyme specific to that reaction, provided by the mitochondrion. Each enzyme also requires one or more cofactors to be present for the associated reaction to proceed efficiently. These enzyme cofactors are supplied via the blood and are none other than the vitamins and minerals we are all familiar with, particularly the B vitamins – thiamine, riboflavin, niacin, folic acid, B12 and others, and minerals like magnesium, zinc, copper, manganese and iron. If anything interferes with this chemical “symphony”, such as a deficiency of one or more of these cofactors, energy production will be impaired and the cell will not be able to function as it should.
Thiamine has been found to have a particularly important role to play. It acts as a cofactor in five of these enzyme moderated reactions, one of which occurs right at the beginning of the whole process, converting the supplied fuel (glucose) into a form usable in subsequent steps. In one of Dr. Lonsdale’s analogies, thiamine is like the spark plugs in an internal combustion engine (the mitochondrion), igniting the fuel/air mixture, turning the released energy into, in this case, mechanical rather than chemical energy, which is used to propel the car (the cell) forward. If the spark plugs are not working properly (if thiamine is deficient), the car will run poorly, if at all.
It is not hard to see the implications of this. At the level of a human being, thiamine deficiency results in beriberi (meaning “weakness”, or “I can’t”). The cells of the body are unable to provide the energy the body needs to function. If the deficiency is not corrected death may follow. At the cellular level, if a virus or bacterium attacks, or if certain cells start to misbehave, the body has cellular defenses to deal with the situation. But if the cells lack energy, these defenses are likely to fail and the body will be overwhelmed. Drs. Lonsdale and Marrs concern themselves with ensuring the mitochondria are in the best shape possible, identifying anything which affects their performance, such as drugs and other chemicals which might cause deficiencies, or genetic defects, and trying to correct such problems generally by means of nutrition, thus maximizing the body’s natural defenses.
This is where the trouble begins. According to Dr. Lonsdale, ever since Louis Pasteur’s discoveries about microorganisms, the paradigm under which medicine has operated is “kill the enemy”, in other words find ways to kill the bacteria and viruses and wayward cells which threaten us with disease, generally using drugs. The idea of helping to strengthen the natural defenses of the body is dismissed out of hand, on the assumption that the issue of nutrient deficiency belongs to the distant past. As the future commander-in-chief of the armed forces of the United States, if one of your military heads came to you and said that you only need offensive weapons and there is no need to worry about the state of your defensive capability, I’m sure that you would send them on their way. Yet that accurately depicts current medical practice. Dr. Lonsdale has for many years tried to persuade his colleagues that thiamine deficiency in particular is a very real problem of the present and the future, particularly in Western societies, for reasons I will go into, and that much of the disease we see is in fact due to it. For his trouble, he has been resolutely ignored, deemed irrelevant and consigned to history by all but a few. All, that is, except perhaps for the many people he has helped. As he tells it, every time he cured someone orthodox medicine had declared incurable, it was put down to “spontaneous remission”.
How I Found Thiamine
I became interested in this subject because of what happened to my elderly mother, now 90. Early in 2019 she came down with a nasty virus. Prior to that she’d had some health problems but was in pretty good shape overall. She recovered but never really got over it. Her longstanding breathing problems became worse. She started to have digestion problems and was back in hospital a few months later with pancreatitis. Back home, every morning after breakfast she had to sit for a few hours because she felt too weak to do anything. On one occasion she had an attack of vertigo, fell and couldn’t get up again. She was seeing several doctors and they were examining her and doing blood tests and trying different drugs on her but I felt they weren’t really helping her much. I resolved to try and work out what was going on. It wasn’t long before I came across Dr. Lonsdale and the subject of thiamine deficiency. What I learnt was that an event that was stressful to the body such as an infection could trigger a state of thiamine deficiency, and that the elderly were particularly vulnerable. I began to think that this was what happened to my mother.
I also had one or two health issues. In 2010, I was diagnosed with thyroid cancer and had it removed. I had occasional heart palpitation episodes, and remembered hearing that the answer for this was vitamin B1. I also have restless legs syndrome. As a result of this new interest in health, I learned about low-carb diets. Around March 2020 I started on a “healthy keto and intermittent fasting” diet and started taking thiamine regularly, along with magnesium, another essential cofactor which is needed for thiamine to work, and encouraged my mother, and my family, to take it. Purely coincidentally, this was also when the COVID crisis was ramping up.
As I learned more, I began to suspect that there was a connection between thiamine deficiency and COVID and that taking thiamine and magnesium might be protective against it. By this time the world was in lockdown, and I thought this would defeat the virus, so there was no need to say anything. By mid-August it was clear that things were spiraling out of control. Around this time, I realized that Drs. Lonsdale and Marrs were very well aware of what was happening and had done what they could to make it known to the world, but it had fallen on deaf ears. I decided I had to try and do something. Having had very little to do with social media, I started using Twitter to try and tell as many people and organizations as I could about the connection between COVID and thiamine deficiency, and have continued doing so to the present, learning more in the process. Everything I have learnt has only strengthened my conviction. Like them, I have had absolutely no response from anyone in a position to be able to do anything and as far as I can tell I have had absolutely no impact and am not going to. I don’t feel like I can just leave it, so that is why I have now turned to you.
Thiamine and Dysautonomia
In 2017, Drs. Lonsdale and Marrs published a book entitled “Thiamine Deficiency Disease, Dysautonomia, and High Calorie Malnutrition”, which more or less represents Dr. Lonsdale’s life’s work. The premise of the book is that thiamine deficiency, beriberi, affects the autonomic nervous system, leading to dysautonomia. The autonomic nervous system controls all of the functions that the body carries out automatically without conscious thought, such as breathing, cardiac function, digestion, sleeping, reacting to stimuli and so on. Basically, this system goes out of whack, resulting in all sorts of strange and seemingly unrelated symptoms particularly affecting the brain, heart, nervous system and digestion. “High calorie malnutrition”, the end result of the typical western diet, is largely responsible.
Beriberi is normally associated with just straight malnutrition or lack of food, and conjures up images of emaciated people. Using the above term Drs. Lonsdale and Marrs are making the point that a diet high in “empty” calories, especially from sugar, but low in micronutrients, predisposes one to the disease, because the available thiamine required to process the fuel is overwhelmed by the amount of fuel being supplied. In terms of the car analogy, the engine is flooded. So the obese could have beriberi. Anyone else nutritionally challenged, such as diabetics, could have it. Basically anyone, young or not, whether they look ill or not, could have it if their nutritional status is compromised. Dr. Lonsdale has for many years been trying to warn us that the Western world is primed for an epidemic of beriberi, waiting for something to come along that would trigger it.
Thiamine, COVID, and an Epidemic of Beriberi
About two weeks after I began tweeting about thiamine, I learned about COVID long-haulers for the first time. These are the people who get over the initial infection, only to find that they continue to have problems for many months afterwards. By now there are perhaps hundreds of thousands in this category. Having learned about the many and varied symptoms of dysautonomia associated with thiamine deficiency, I was stunned to realize that the symptoms of long-haulers, described in an endless succession of media reports as the bizarre and mysterious symptoms of COVID, are exactly the same as those of mild thiamine deficiency. Despite my numerous efforts to point this out, such reports continue to appear to this day. Of course when I checked back with what Dr. Marrs had been saying on Twitter, I found she was already pointing all this out months earlier.
To me the implications of this are enormous. It suggests that the world has completely misunderstood the nature of the pandemic and as a result of this wrong understanding the wrong decisions are being made. While undoubtedly highly contagious, I believe COVID is not the highly novel, pathogenic and virulent virus we are led to believe. Rather it is similar to, but somewhat more severe than, what we have experienced previously, the effect of which has been to unleash an epidemic of, not the version we know from history, but a modern-day equivalent form of beriberi, attributable to our generally poor nutritional status and any other environmental contributors to poor mitochondrial function.
As one example of the decisions being made, one could consider what has been happening in intensive care units around the world. Perhaps the most characteristic aspect of COVID is loss of pulmonary function, known as Acute Respiratory Distress Syndrome (ARDS). While I am no expert, it seems an assumption being made is that to overcome this just requires an increased supply of oxygen by means of a ventilator. Earlier I described respiration as it takes place at the cellular level. In terms of normal combustion everyone knows one needs three things: fuel, oxygen, and a source of ignition. It’s the same at the cellular level – it’s not enough to have glucose and oxygen, you need thiamine to act as the spark plug, followed by the chain of reactions that take place inside the mitochondrion. Perhaps thiamine deficiency, and therefore failure to initiate this reaction chain, rather than lack of oxygen, is what’s really going on. While I could find numerous general references to the use of thiamine in clinical care, when I looked at ICU protocols specifically for COVID promulgated by organizations such as WHO and CDC and in Australia, I did not find any reference to using thiamine.
There are other observations one can make. One of the seemingly mysterious features of the pandemic is that many people who get infected are completely asymptomatic. I interpret this as meaning these people have good nutritional status, and mitochondria that are working efficiently, and their cellular defenses are consequently able to deal with the virus. Also, people with a lower socioeconomic background seem to be more severely affected. This is understandable as they might only have access to cheaper, less nutritious food and are therefore more likely to be in a state of incipient thiamine deficiency when they encounter the virus. And of course, as Boris Johnson learned and as many doctors are starting to understand, a poor diet, despite access to plenty of food, leading to obesity, makes one vulnerable, the answer being to improve the diet, which doctor Lonsdale tells us should be a low carbohydrate, “real food” diet, which even now is not what nutrition guidelines recommend.
Consider Thiamine
This brings me to the main purpose of this letter. In the absence of, or in addition to, a vaccine, I believe that an emergency program of mass daily supplementation with thiamine and magnesium, and a longer term aim of improved diet, could help to protect the U.S. and indeed the world population, from the virus. One might put it as a policy goal of ensuring thiamine sufficiency in the general population. This could provide an alternative to the devastating human and economic consequences of the actions currently being taken or contemplated, whether lockdowns, border closures, or so-called “herd immunity” options. I imagine this would be a very large undertaking, more than just education as this would probably result in all existing supplies vanishing, but presumably much less than the expected vaccination program, given that both micronutrients are well-known, cheap and non-toxic. Of course, all this would need to be verified before taking action. If one can measure the level of intracellular thiamine sufficiency or deficiency in the body it should be straightforward to test hypotheses, e.g. that long-haulers are in a state of deficiency, that those who were asymptomatic have a good level of sufficiency, and so on. One difficulty with this is apparently that because of the lack of interest in this subject there is currently almost no laboratory where such measurements can be made.
The Stress of Illness
It was only a couple of weeks ago that I realized Dr. Lonsdale actually made this suggestion himself. In an article published on March 20, 2020 on the Hormones Matter website, entitled “What Can Selye Tell Us About COVID-19? Survival Requires Energy”, he said:
We believe that we have shown evidence that thiamine and magnesium supplementation are inherently necessary in a population in which nutrition is imperfect. … Moreover, if we consider the requisite ‘energy’ required to stave off any illness, might we also consider bolstering the nutrient stores e.g. host defense in at-risk populations, as a way to reduce the risk and severity of the illness? Doing so may help ensure the adequacy of energy in meeting the unseen enemy.
You will recall that this was right at the beginning of the period when deaths started to ramp up in the U.S. One wonders how different things might have been if he had been listened to.
The biggest challenge, however, could lie elsewhere. This pandemic has brought us to an extraordinary place. Suppose that Dr. Lonsdale is right. This gives rise to an incredible dichotomy. On one side there is 96 year old Dr. Lonsdale, who has few resources and at his age may not be in a position to advocate for himself, but who with a vast amount of experience behind him has a simple idea that explains an awful lot, including many diseases which medical orthodoxy cannot explain or treat, which therefore get labelled psychosomatic. He has a proposal which is easily testable, could easily be trialled, is simple and relatively cheap to implement, and could have enormous health and economic benefits. Without going into details, it could potentially lead to generally improved mental health, reduced levels of crime and reduced vulnerability to virtually all forms of disease, including viral threats that we have yet to encounter, with consequently greatly reduced health costs and productivity benefits for all economies. This would usher in a science based health renaissance, the likes of which has never been seen before.
On the other side is the entire medical establishment with its vast resources, having an entrenched position, which is unable to, indeed cannot afford to, so much as entertain the possibility that Dr. Lonsdale could be correct. You also have the pharmaceutical industry pouring billions into drug development and searching for a vaccine. A vaccine may well be found, which might head off this crisis of credibility. Or it may not. Or the virus may mutate regularly, rendering a vaccine next to impossible as with cold viruses. One thing to note is that, if the pandemic at its core is the result of a nutrient deficiency, then no drug or combination of drugs that does not correct the deficiency can possibly overcome it. On top of that, you have the food industry with its vested interests in keeping the world hooked on its cheaply made, highly addictive products based on sugar and processed carbohydrates, which Dr. Lonsdale tells us lies at the core of the problem. The pandemic is forcing us to face the inconvenient truth that this entire edifice may be unsustainable.
I’m sure you can appreciate why I think you may be the only person who might have a chance of getting us from where we are to where we could be. I’m sure you would have people to advise you on health matters. If Dr. Lonsdale is right, and you ask them for advice on this, it seems likely they will just dismiss the entire notion out of hand. If we are to avoid unthinkable levels of human and economic loss, you may have to shake the foundations of the medical establishment to its very core, to get it to accept that we need defense as well as offense in order to successfully do battle with the invisible enemy.
In the end, it may simply be a matter of going back to where it all began – back to Hippocrates, who, as Dr. Lonsdale likes to remind us, said “Let food be thy medicine and medicine be thy food.”
A Few Final Observations
I hope you get to meet Dr. Lonsdale. I strongly suspect the fact that he is still active at such an advanced age is not an accident. I imagine he has been taking his own advice. I would not be at all surprised to learn that he has lived most of his life without any significant disease. I would very much like to see him get the recognition he deserves before he dies.
If I’m right about thiamine deficiency leading to weakness in the response of cellular defenses, this could have an impact on the effectiveness of any vaccine that may be developed, since it has to piggyback on the existing cellular mechanisms. It may turn out that the underlying problem of thiamine deficiency has to be recognized and addressed even if a vaccine is produced.
I am very much a layman, so am not someone from whom to seek advice. If I hear that you are interested in pursuing this I will let Dr. Marrs know. She would be the best person to contact in the first instance.
Lastly, it seems to me that, if dealt with wisely, this has the potential to demolish the foundations of the incredible tower of disinformation that besets the American people and bring it crashing to the ground, perhaps ushering in a new, sorely lacking respect for science. Exactly how and when that might be brought about I have no idea. I’ll leave that up to you.
Good luck in your new adventure.
Robert Olney
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, like it, please help support it. Contribute now.



You might be interested in