
A while back, a friend of mine shared a story on Facebook about a doctor’s nonchalant response to side effects experienced by a patient on birth control. I commented that this was one of my least favorite among the common phrases doctors use to gaslight women.
That friend was Sara Harris, who is doing amazing work getting the word out about Fertility Awareness Methods and helping women with hormone issues in Australia with her podcast, Follow Your Flow. Sara knew I was wrapping up work on a new, expanded audio version of my book and recommended I visit her podcast again to promote the audiobook and present my ‘Top 10 Least Favorite Things Doctors Say About Birth Control.’ You can listen to the resulting podcast here.
Lack of Respect
Obviously, I took her up on the offer, burning a lot of energy to get my Top 10 in the proper order – only to change that order and change it again the more I contemplated each phrase. Ultimately, I felt like I could have just as easily said they were in no particular order because each dismissive phrase poses its own set of disturbing problems.
For the purpose of this article, I want to focus on three of these statements, which are particularly egregious in their lack of respect for the potent drugs delivered by hormonal birth control and the detrimental impact they have on women’s health.
And so, here are those three statements… this time, in no particular order.
Localized Hormones
“This birth control option is safer because the hormones are localized.”
Doctors tend to offer this falsehood when speaking about either NuvaRing or the hormonal IUD. It is frequently used to sell a young woman on using the device, but it’s also used later to dismiss questions she may have about side effects she develops after insertion.
I have trouble believing that a medical doctor actually believes that these hormones camp out in the uterus and just manage fertility. Hormones are systemic. By their very nature, they travel throughout the body attaching to hormone receptors that reside on every cell in our bodies.
Now, here’s the kicker – not only are these drugs not localized, but they have the potential to be even more dangerous than hormones that are taken by mouth. Oral contraceptives (as with any drug taken orally) are processed through the digestive system in what is known as first-pass metabolism. This process reduces the concentration of active drug prior to being introduced into the blood stream.
Consequently, drugs distributed via the uterus bypass this first-pass metabolism thereby reaching the bloodstream more quickly and in a more potent state.
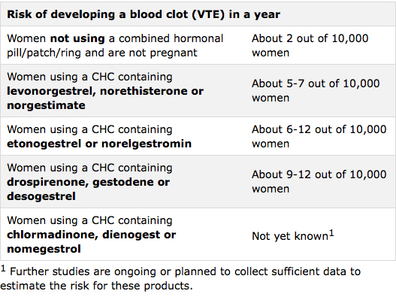
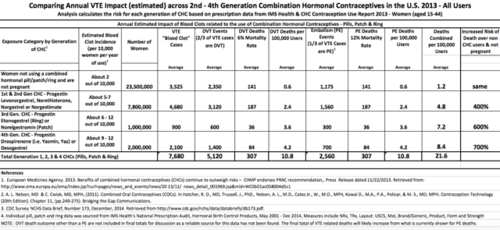
It shouldn’t be surprising then that a recent Danish study found that women on NuvaRing were six times more likely to develop a deep vein thrombosis than women not taking birth control, and twice as likely as women taking a combination pill.
Psychotropic Candy
“Don’t worry. I’ll just prescribe an antidepressant to go with your birth control.”
Many doctors seem to think antidepressants can be used to accommodate just about any symptom manifested as a result of birth control. In my book, In the Name of The Pill, I shared the story of a young woman with lupus.
After quitting hormonal birth control, her lupus symptoms became surprisingly manageable. This continued for a few years, until she decided to try a different formulation of birth control. Shortly after starting The Pill again, her lupus symptoms came roaring back. But, when she told her doctor about it, he didn’t think the birth control had anything to do with her flare-ups.
He advised her to keep taking it and prescribed her an antidepressant to ‘help her rest better.’
I believe doctors who pull stunts like this have lost any sense of respect for the potency of the drugs they are doling out. This goes for any drug – not just birth control. As one of the doctors Barbara Seaman quoted in her landmark book, A Doctors’ Case Against the Pill, warned, “It needs to be emphasized that if you give a patient one drug and counteract it with another, there is a rising curve of adverse reactions.”
In my opinion, this warning should be doubled where birth control is concerned because the powerful drug is essentially being used to treat pregnancy rather than some life-threatening disease. As Mayo-trained, Dr. Philip Ball put it at the Nelson Pill Hearings, “I believe that we physicians are so used to administering very potent medications to very serious disease problems, we have not really yet learned, it is a totally different circumstance to administer powerful but nonessential drugs chronically to healthy young women.”
You can read more about specific concerns related to the mixture of psychotropic drugs and hormonal birth control here.
Suddenly Supplements
The third comment deals exclusively with the Depo injection and needs a little setup. The FDA requires a black box warning on this drug’s information pamphlet. A warning in big, bold letters accentuated by a thick, black frame states:
“WARNING: LOSS OF BONE MINERAL DENSITY”
The warning goes on to explain that your bone loss will be greater the longer you take the product and these changes may be irreversible. It reinforces these concerns by stating that Depo should not be used as a long-term birth control solution, even capping its recommended use at no more than two years.
That seems pretty clear and absolute, but many women who have asked their doctors about this warning have been told:
“Just take a calcium supplement, and you’ll be fine.”
Mind you, the FDA warning says nothing about taking a supplement to offset the affects. In fact, it doesn’t suggest there are any measures you could take to avoid the potential consequences.
The FDA is a slow-moving, bureaucratic government agency. It takes a lot of evidence to overcome the inertia associated with issuing such a dramatic black box warning. For a doctor to ignore or deny such a warning and suggest the solution is as easy as taking a calcium supplement is borderline criminal.
Health as a Business
If your doctor ever uses any of these three lines, you should seriously question his/her motivation. Do they care about your health or do they see your healthcare as a business?
One of the things I frequently tell women is to trust your questions more than the answers. If you mention a side effect that concerns you, and your doctor seems more interested in convincing you The Pill had nothing to do with it, don’t assume you’re crazy or you’re the only one experiencing this. Your body is sending you this warning sign for a reason. Keep questioning.
I once had an Ob/Gyn tell me that it’s difficult to get anyone from her specialty to say anything bad about hormonal contraceptives because it represents about a third of their business.
However, if you are a medical professional who recognizes that birth control is much more dangerous than women are being led to believe, be proactive in sharing that information, even if you aren’t an Ob/Gyn.
Women need to hear it. Many feel isolated. They’re afraid to discuss their side effects because they think they’re the only ones having a bad experience. Or worse, they wonder if they may be going crazy.
An eye surgeon recently reached out to me and shared what’s been happening at her practice after she read my book. She said she always takes a complete medical history, part of which includes the patient’s use of hormonal contraceptives. Lately, even though she doesn’t deal directly with menstrual issues, when a woman reports certain ‘mysterious, undiagnosable symptoms,’ this doctor has started recommending they stop taking their birth control. She said a few patients have already contacted the office to thank her because their symptoms have improved dramatically.
I hope more physicians will hop on board and fearlessly tell women about the myriad side effects of birth control. We still have a ways to go, but maybe someday I will be able to compile a list of my Top 10 Favorite Things Doctors Say About Birth Control.
The FDA approved The Pill despite it not being proven safe. Today, it has been linked to everything from blood clots and cancer to lupus and Crohn’s disease — and still has not been proven safe.
This book explores the medical and historical disconnects that brought us to this point.
Last updated on October 21, 2023 at 9:38 pm – Image source: Amazon Affiliate Program. All statements without guarantee.
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, like it, please help support it. Contribute now.
Yes, I would like to support Hormones Matter.
This article was published originally on December 13, 2021.



You might be interested in


































{kind=link}