Poor Nutrition Stress: The Enemy of Health

In previous posts, I have indicated that stress can initiate or exacerbate disease and medication or vaccine adverse reactions. Read that statement, you might think I am attributing the onset of serious disease and adverse reactions to a psychosocial cause. That is not the case. Stress comes in a myriad of forms, some external, some internal, and although much of what we call stress relates to psychosocial responses to perceived threats, I think stress encapsulates so much more. At its most fundamental level, stress represents a physical state where the body is performing less than optimally. Let me explain.
What is Stress?
I define the word “stress” as a physical or mental force that is acting upon you. An example of mental or psychosocial stress might be an insult from a person, meaning that the stress comes from a source outside the body. On the other hand, it might be the realization that a deadline has to be met, a mental source from within. Any form of injury is an obvious source of physical stress. Physical action such as shoveling snow is another form of stress, demanding energy consumption imposed by the individual who wishes to get rid of the snow. Being infected with a virus or by bacteria is a form of stress that demands a defensive reaction. In each of these instances, the body reacts to the inflicting stressor. Sometimes, when the resources are available, it reacts efficiently. Other times, when the resources are not available or when additional factors intercede, the body’s response to the stress is ill-adapted.
Your Body is Your Fortress, Your Immune System the Soldiers
Perhaps an analogy might help to provide an explanation for the remarks that follow. I imagine the body as being like an old fashioned fortress. The people living within it go into action when the fortress is attacked by an enemy from outside. It would be of little use if the defense soldiers went to the eastern battlements if the attack came from the west and so there had to be a central figure that would coordinate the defensive reaction. The nature of the attack would be spotted by a guard on duty and the central figure informed by messenger.
The body represents the fortress and the lower part of the brain represents the central figure that coordinates the defense. The cells in the blood known as white cells can be thought of as soldiers, armed with the necessary weapons to meet the nature of the enemy. Suppose, for example, a person’s finger is stuck by a splinter carrying a disease bearing germ. The pain, felt in the brain, recognizes its source and interprets it as a signal that an attack has occurred. White cells in the area can be regarded as the “militia under local command” and a “beachhead” is formed to wall off the attack. The white cells sacrifice themselves and as they die, they form what we call pus. If the beachhead is broken and the germs manage to get into the bloodstream, it is then called septicemia and the brain/body goes into a full defensive reaction where high fever is the most obvious result. Such an illness is an attack/defense battle.
The symptoms that develop from such an infection represent the evidence for this defense, feeling ill, pain and developing a fever are excellent examples. Micro-organisms are most efficient at 37° C, the normal body temperature. The rise in body temperature, initiated by the brain, makes the microorganisms less efficient and may kill some of them. One therefore has to question the time honored method of reducing the fever, during illness, as being an example of good treatment. While reducing fever improves the symptoms caused by the infection, it also reduces the efficiency of the immune battle raging within.
The outcome against the stressor is death or recovery; although it is possible sometimes to end up in a kind of stalemate, represented by prolonged symptoms of ill health. Chronic illness may be viewed as the immune system’s inability to eradicate fully the stressor.
Poor Nutrition and Stress
As I have emphasized in previous posts, the autonomic (automatic) nervous and endocrine systems are used to carry the messages between the body and the brain that enable the defense to be coordinated. This demands a colossal amount of cellular energy, no matter the nature of the stress. That energy to fight stress comes from oxidation of the fuel that is provided from nutrition. Of course, the greater the stress the greater the energy demand, but in the end the equation is quite simple. If the energy required to meet the stress is greater than the energy that is supplied, there must be a variable degree of collapse within the defensive system. That collapse presents as intractable symptoms, where the body is unable provide the energy needed to sustain health. This is the secret of the autonomic dysfunction in the vitamin B1 deficiency disease, beriberi. It is also the secret behind the initiation of POTS because both conditions are examples of defective oxidation. You can read more details regarding thiamine deficiency, beriberi, POTS and other health issues from previous posts on this website
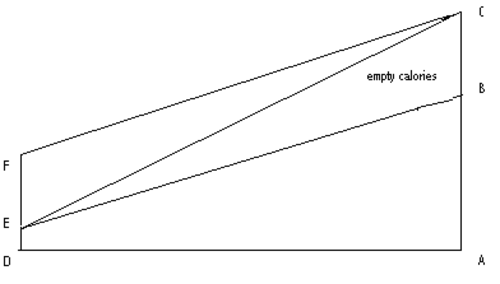
High Energy Demands Equal High Nutritional Demands
Nutrient density of diet might appear to be perfectly adequate for a given individual, but inadequate to meet the self-initiated energy demands of a superior brain/body combination in a highly active individual such as an actively engaged student or athlete. Our genetic characteristics, the quality of nutrition and the nature of life stresses each represent a factor that all combine together to give us a profile for understanding health and its potential breakdown.
Epigenetics and Mitochondria: The Stress of Our Parents
Epigenetics, the science of how our genes are influenced by diet and lifestyle, is relatively new. Epigenetics considers the possibility that genes can be activated and deactivated by nutrition and lifestyle. Stress can come in many forms, from psychosocial trauma, poor nutrition, environmental and medical toxin exposures, to infections. Stress impacts how our genes behave. Even though one may inherit a hard-coded genetic mutation from a parent, that mutation may not be activated unless exposed to a particular type of stress. Similarly, an individual who may have no obvious illness-causing genetic abnormalities but stress, in the form of nutritional depletion, exposures or trauma, can turn on or turn off a set of genes that induce illness. What is remarkable about epigenetics is the transgenerational nature of the stressors. The memories of stressors affecting our parents and even our grandparents can affect our health by activating or deactivating gene programs.
We also have to consider the state of our mitochondria, the “engines” in each of our cells that produce the energy for cellular function (to learn more about mitochondria and health, see previous posts on this website). Mitochondria have their own genes that are inherited only from the mother. Damage to the DNA that makes up these genes sometimes explains the similarity of symptoms that affect a given mother and any or all of her children. For example, although this damage may be inherited, we also have scientific evidence that thiamine deficiency, known to be the result of poor diet, can damage mitochondria. A bad gene might be the solitary cause of a given disease, but even where this is known as the cause, the symptoms of the disease are sometimes delayed for many years, suggesting that other variables must play a part. A minor change in cellular genetic DNA might be alright to meet the demands of normal living, but impose a risk factor that could be impacted by prolonged stress or poor nutrition, and disease emerges.
Nutrition is the Only Factor that We can Control
The imposition of stress on any given individual is variable, most of which is accidental and out of our control. Therefore, if we represent these three factors, genetics, stress and nutrition as three interlocking circles, all of which overlap at the center of such a figure, there is actually only one circle over which we have control and that is nutrition. We now know from the science of epigenetics that nutritional inadequacy can affect our genes. By examining the mechanism by which we defend ourselves against stress, we can also see the effect of poor nutrition.
Poor Nutrition Equals a Poor Stress Response
Using these three variables, perhaps we can begin to understand several unanswered questions. Why does a vaccination negatively affect a relatively small percentage of the total population vaccinated? Or why do some medications negatively impact only some individuals? It might be because of a genetic risk factor or because of a collapse of the coordinated stress response related to quality of nutrition or a combination of both. Why does a vaccination tend to “pick off” the higher quality students and athletes? Again, the same kind of answer; high quality machinery demands high quality fuel. Since the limbic system of the brain has a high energy demand and represents the computer that coordinates a stress response we can understand the appearance of beriberi or POTS and cerebellar ataxia, all examples of a deviant response to stress. Nutrition, therefore, should not be looked at as supplement to good health, but as the foundation of health. When disease or medication and vaccine reactions emerge, efforts to identify and then restore nutritional deficiencies must be the first line of immune system health. Without critical nutrients, the body simply cannot mount a successful stress response and the battlefield will expand and eventually fall.
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, like it, please help support it. Contribute now.
Yes, I would like to support Hormones Matter.
Image by Pedro Figueras from Pixabay.



You might be interested in